
More Information
Submitted: August 12, 2024 | Approved: August 19, 2024 | Published: August 20, 2024
How to cite this article: Sheth U, Lee J, Nam D, Henry P. The Effect of Shoulder Immobilization Position on Outcomes Following Rotator Cuff Repair: A Scoping Review. J Sports Med Ther. 2024; 9(3): 060-067. Available from: https://dx.doi.org/10.29328/journal.jsmt.1001084
DOI: 10.29328/journal.jsmt.1001084
Copyright License: © 2024 Sheth U, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Abduction brace; Sling; Rotator cuff repair

The Effect of Shoulder Immobilization Position on Outcomes Following Rotator Cuff Repair: A Scoping Review
Ujash Sheth* , James Lee, Diane Nam and Patrick Henry
, James Lee, Diane Nam and Patrick Henry
University of Toronto Sports Medicine (UTOSM) Program at Women’s College Hospital, Toronto, Ontario, Canada
*Address for Correspondence: Ujash Sheth, University of Toronto Sports Medicine (UTOSM) Program at Women’s College Hospital, 2075 Bayview Avenue, MG 352, Toronto, ON, M4N 3M5, Ontario, Canada, Email: [email protected]
Introduction: There has been growing interest in determining the influence of post-operative immobilization posture and rehabilitation protocol on healing rates and clinical outcomes. Current consensus calls for the use of an immobilization device post-operatively, which commonly comes in the form of a standard sling or an abduction brace with the arm positioned in varying degrees of abduction. There is a lack of high-level evidence in the literature to recommend one type of immobilization device or arm position over another.
Objectives: This study aimed to summarize the current clinical and biomechanical evidence for the optimal postoperative positioning and bracing of the arm following arthroscopic rotator cuff repair.
Methods: A comprehensive search of the electronic databases EMBASE, MEDLINE, and PubMed was performed using a combination of the following keywords and medical subject heading (MeSH) terms: ‘arthroscopic’, ‘rotator cuff repair’, ‘sling’, ‘brace’ and ‘immobilization’. This systematic review was conducted following the Preferred Reporting for Systematic Reviews and Meta-analysis (PRIMSA) guidelines. Two reviewers performed an independent assessment of the methodological quality of each eligible clinical study using the Methodological Index for Non-Randomized Studies (MINORS).
Results: Based on current biomechanical evidence, placement of the arm into an abducted position following rotator cuff repair was found to be favorable. An abduction angle of 30° was associated with lower strain on the repair while maintaining appropriate contact pressure at the footprint. However, the use of an abduction brace did not result in a clinically significant improvement in long-term PROM, ROM, and re-tear rates when compared to a traditional sling in clinical studies.
Conclusion: Despite observing favorable outcomes with abduction bracing after rotator cuff repair in biomechanical studies these findings were not reproduced in clinical studies. However, current clinical studies are comprised of small sample sizes, varying tear sizes, and significant heterogeneity in both, the degree of abduction and forearm rotation. Future studies should be directed towards prospectively investigating the effect of immobilization position among patients with similar rotator cuff tear sizes.
Rotator cuff tears are the most common source of shoulder pain and disabilities [1-3]. As a result, arthroscopic rotator cuff repair has become one of the most frequently performed orthopedic procedures [4,5]. However, rotator cuff repairs have historically been associated with high re-tear rates ranging up to 70% [6-10]. A variety of biomechanical and clinical studies have attempted to identify factors influencing outcomes following rotator cuff repair. As such, there has been growing interest in determining the influence of post-operative immobilization posture on healing rates and clinical outcomes [6,7,11-20]. Current consensus calls for the use of an immobilization device post-operatively, which commonly comes in the form of a standard sling with the elbow flexed to 90o and the arm internally rotated at the side of the body or an abduction brace with the arm positioned in varying degrees of abduction. However, there is a lack of high-level clinical evidence in the literature to recommend one type of immobilization device or arm position over another [21]. This study aimed to summarize the current clinical and biomechanical evidence for the optimal postoperative positioning and bracing of the arm following arthroscopic rotator cuff repair.
This systematic review was conducted following the Preferred Reporting for Systematic Reviews and Meta-analysis (PRIMSA) guidelines [22]. Ethics board approval was not required as the study was based on a review of already published literature.
Literature search & study selection
A comprehensive search of the electronic databases EMBASE, MEDLINE, and PubMed was performed using a combination of the following keywords and medical subject heading (MeSH) terms: ‘arthroscopic’, ‘rotator cuff repair’, ‘sling’, ‘brace’ and ‘immobilization’. Titles, abstracts, and full texts were screened in duplicate by two independent reviewers (JL and US). References of included studies were reviewed for additional relevant articles that met the criteria for inclusion. Duplicates were manually excluded. Disagreements were resolved by a consensus decision with a third reviewer (PH).
Eligibility criteria
Studies were eligible for inclusion if they evaluated the influence of postoperative immobilization technique on clinical and radiological outcomes following arthroscopic rotator cuff repair. Biomechanical and clinical studies were included. Review articles, expert opinions, and technique studies were excluded. The search was limited to English-language articles.
Data extraction
Data was extracted independently by two reviewers (JL and US). Data collected from clinical studies included: author, year of publication, demographic variables, immobilization technique and device used, postoperative rehabilitation protocol, mean length of follow-up, patient-reported outcomes, and other notable results. Data collected from biomechanical studies included tear characteristics, repair technique, and tension and strain at various arm positions.
Assessment of risk of bias of eligible studies
Two reviewers performed an independent assessment of the methodological quality of each eligible clinical study using the Methodological Index for Non-Randomized Studies (MINORS) [23]. The MINORS criteria is a validated 12-item scale designed to assess the methodological quality of non-randomized surgical studies, including both non-comparative and comparative studies [23], Appendix A.
| Appendix A | |||||||||||||
| Study | A clearly stated aim | Inclusion of consecutive patients | Prospective collection of data | Endpoint appropriate to the aim of the study | Unbiased assessment of the study endpoint | Follow-up period appropriate to the aim of the study | Loss of follow-up less than 5% | Prospective calculation of the study size | Additional Criteria for Comparative Studies | ||||
| An adequate control group | Contemporary group | Baseline equivalence of groups | Adequate statistical analysis | Total ( /24)* ( /16)^ |
|||||||||
| Hollman, et al 2017 (32) | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 22 |
| McColl, et al 2019 (33) | 2 | 2 | 2 | 1 | 1 | 0 | 1 | 2 | 11 | ||||
| Conti, et al 2014 (34) | 2 | 2 | 2 | 1 | 1 | 1 | 2 | 2 | 1 | 2 | 1 | 2 | 19 |
| Ghandour et al. 2019 (35) | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 22 |
| Silverio, et al 2014 (36) | 2 | 2 | 2 | 2 | 2 | 2 | 1 | 2 | 15 | ||||
| Pandey et al 2020 (37)_ | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 2 | 22 |
| *Maximum possible score for comparative studies ^Maximum possible score for noncomparative studies |
|||||||||||||
Statistical analysis
Statistical analysis was performed to summarize all continuous and categorical data. No inferential statistical testing was performed.
Study characteristics
Among the 32 full-text articles reviewed, a total of 15 studies were deemed eligible based on our inclusion and exclusion criteria (Figure 1). The included studies comprised nine biomechanical studies [6,24-31] (Tables 1,2) and six clinical studies [32-37] (Table 3) examining outcomes with sling and abduction brace use following arthroscopic rotator cuff repair.
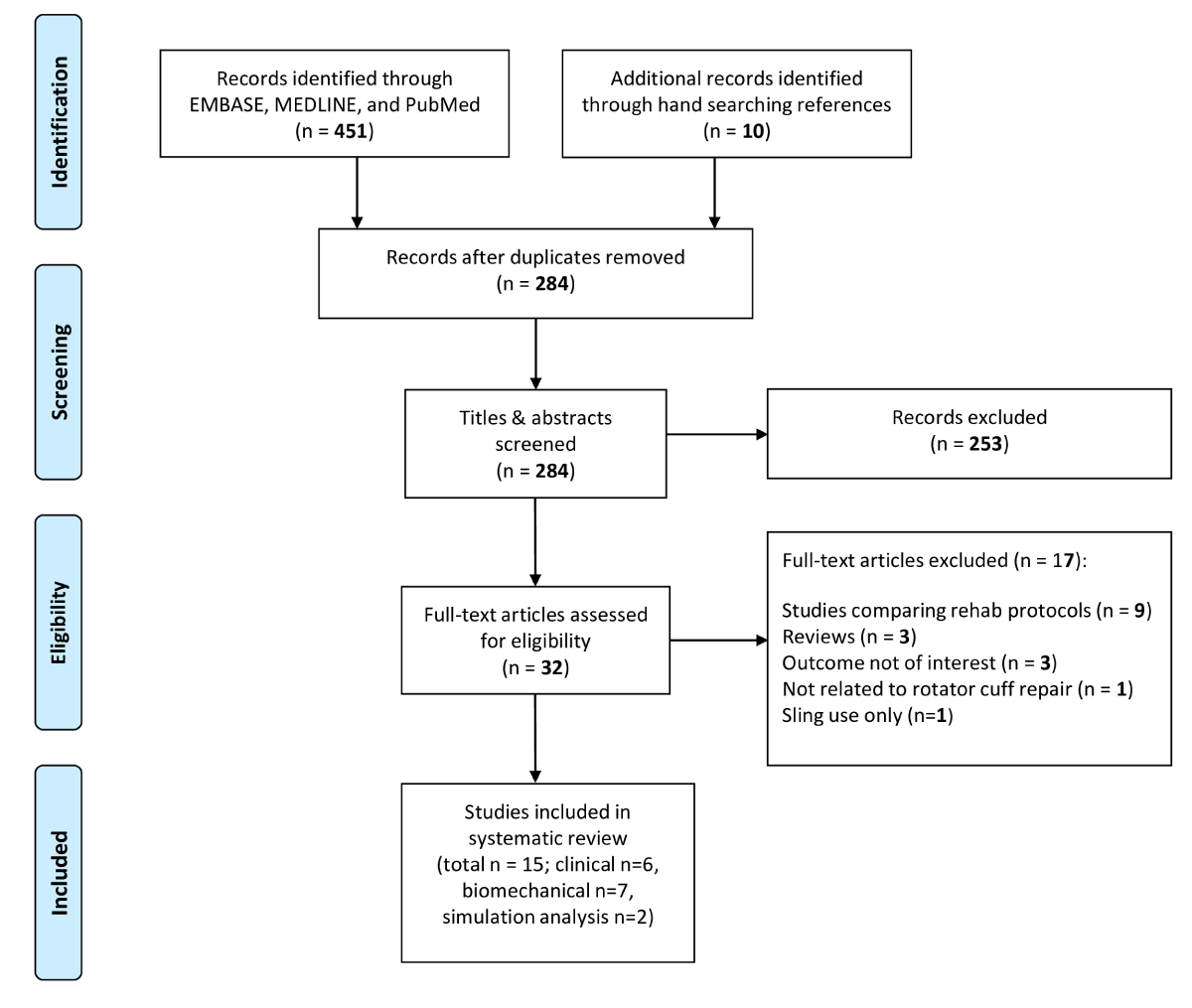
Figure 1:
| Table 1: Summary of biomechanical studies examining effect of shoulder position on rotator cuff repair strain. | |||||
| Authors | Year | Specimens | Tear Characteristics | Rotator Cuff Repair Technique | Findings |
| Zuckerman, et al. [24] | 1991 | 12 fresh frozen human shoulders | "Small": Entire width of tendon + 1 cm length of supraspinatus (full-thickness) | Open; #2 Mersilene tape; horizontal mattress | Unchanged tension (N < 2) with abduction 30,60,90,120° Increase in tension with Abduction decreased to 15° (p < 0.01) |
| "Large": Entire width of tendon and + 2 cm length of infra and supraspinatus (full-thickness) | Open; #2 Mersilene tape; horizontal mattress | Stable strain regardless of rotation, at flexion/extension above 30° degrees abduction. | |||
| Hatakeyama, et al. [25] | 2001 | 14 fresh frozen human shoulders | 2 cm width X 1.5 cm length, full thickness of supraspinatus | Open; #2 braided non-absorbable sutures, trans-osseous | Increased strain with decrease in elevation in scapular plane 30 to 15° and 15 to 0° (p < 0.01). With arm elevated 30 degrees in scapular plane, average tensile force < 0.3 kg at any rotation. |
| Reilly, et al. [26] | 2004 | 3 cadaveric human shoulders | Full thickness supraspinatus tendon tears with 2 cm retraction | Open; #2 Ethibond, transosseous Mason-Allen | Mean reduction of tension by 34.1N as shoulder taken from 0 to 30° abduction |
| Andarawis-Puri, et al. [27] | 2009 | 10 fresh frozen human shoulders | 33% bursal, 66% bursal, full thickness supraspinatus tendon | Open; 1) #2 fiber-wire; Modified Mason-Allen transosseous 2) horizontal mattress with 2 suture anchors | Lowest strain at 30° abduction for all types of supraspinatus tears. Lowest strain of both infra and supraspinatus tendon at 30° abduction. |
| Howe, et al. [28] | 2009 | 6 fresh frozen human shoulders | Full thickness supraspinatus tendon tear | Open; #2 Ticron, transosseous horizontal mattress | Arm externally rotated 30°: tension in the anterior suture 10X posterior suture (p < .001). Arm internally rotated 30°: tension in the posterior suture 10X that of anterior suture (p < .0005). No significant difference in the suture tension with arm in neutral rotation. |
| Park, et al. [38] | 2009 | 6 fresh frozen human shoulders | Entire width of tendon + 1cm length, full thickness of supraspinatus | Open; #2 Fiberwire suture anchors 1) Modified double row 2) Double-row 3) Single row | Decreasing footprint contact pressures and contact area with increasing abduction Abduction < 30 and internal rotation to 60 most optimal footprint contact. Overall, the results favour the arm in 0° to 30° of abduction. |
| Hawthorne, et al. [29] | 2018 | 4 fresh frozen human shoulders | Full thickness supraspinatus tendon | Open, Two knotless anchors, single row, inverted mattress | Decrease in anterior and posterior tendon strain and posterior increasing abduction angle Small abduction pillow caused a reduction in tension on the supraspinatus of 27% anteriorly and 55% posteriorly compared to placing the shoulder in the position of a sling without an abduction pillow A large abduction pillow caused a further reduction in tension, of 42% anteriorly and 56% posteriorly |
| Table 2: Summary of simulation studies examining the effect of shoulder position on rotator cuff repair strain. | ||||
| Author | Year | Model | Tear Characteristics | Findings |
| Jackson, et al. [30] | 2013 | Computational shoulder model | Gap length 0 mm - 20 mm of (1) full-thickness supraspinatus tears, (2) full-thickness supraspinatus and infraspinatus tears, and (3) full-thickness supraspinatus and subscapularis tears. |
Optimal position for isolated supraspinatus tear: humeral elevation 61 to 109 degrees as tear 13 to 37° anterior to the coronal plane with neutral or internal rotation (76% to 90% stress reduction). Optimal position for supra + infraspinatus tears: elevation between scapular and coronal plane 61 to 106 degrees with neutral to limited internal rotation (76% - 83% stress reduction for the supraspinatus and 29% - 47% for the infraspinatus). More anterior elevation plane optimal with subscapularis tear |
| Saul, et al. [31] | 2011 | Computational shoulder model | Gap length 5mm to 30mm of supraspinatus | Passive force from 28.5N to 518.1N when shoulder position was changed from 60 to 0° of shoulder abduction, for rotator cuff with 0.5 cm gap |
Study characteristics
Among the six clinical studies included in our review, there were a total of 1868 patients [32-37]. A total of three randomized controlled trials [32,34,37], two prospective cohorts [33,36], and one retrospective cohort study [35] were included. The mean age of patients was 58.7 ± 2.2 years, while 54.4% were male. Four studies [33,34,36,37] had a minimum follow-up of 12 months. Two studies reported at least 6 months of follow-up [32,35]. All included studies permitted pendular exercises during the immediate postoperative period, with the initiation of active range of motion at the 6-week postoperative time point (Table 3). The overall risk of bias in clinical studies was low. MINORS score ranged from 19 to 22 out of a maximum score of 24 in comparative studies and 11 to 15 out of a maximum score of 16 in non-comparative studies [32-37].
| Table 3: Clinical studies investigating sling and abduction brace use for rotator cuff repair. | |||||||||||
| Study | Year | Level of Evidence |
Immobilization Method | Duration of immobilization (weeks) | Sample Size (N) | Age (SD) | Sex (M:F) | Minimum Follow-up (months) | Rotator Cuff Repair Technique | Rehab Protocol | Outcomes |
| Conti, et al. [32] | 2015 | Internal Rotation (15°) Sling | 6 | 20 | 62.3 ± 5.8 | NR | 6 | Single Row | Immediate: Pendulum and pROM; aROM 6 weeks | ROM, UCLA, DASH, VAS, SST, Constant | |
| I | External Rotation (15°) + Abduction Brace (15°) | 6 | 20 | 59 ± 7.0 | NR | 6 | |||||
| Silverio, et al. [33] | 2014 | II | Abduction Brace | 6 | 45 | 64 ± 17.3 | 20:25 | 12 | NR | Pendulum for 6 weeks, 1 hour out of brace | ASES, SST, UCLA, Adherence |
| Hollman, et al. [34] | 2017 | Anti-Rotation Sling | 6 | 16 | 62.5 ± 9.76 | 5:11 | 12 | Double Row (29); Single Row (7) | Immediate: Pendulum, restricted passive ROM; aROM starting 6 weeks | VAS, CMS, WORC, ROM, satisfaction, EQ-5D-3L | |
| I | Abduction Brace (30-40°) | 6 | 20 | 60.2 ± 6.84 | 11: 9 | 12 | |||||
| McColl, et al. [35] | 2019 | III | Abduction Brace | 6 | 1600 | 59 ± 0.3 | 883: 717 | 6 | Single Row | Initially immediate pROM, and aROM at day 8; Less aggressive as study progressed | Retear Incidence (ultrasound) |
| Ghandour, et al. [36] | 2019 | Open Pouch Sling | 6 | 55 | 50.8 ± 12.0 | 28:27 | 12 | Double Row |
pROM 6 weeks, aROM after | VAS, CMS | |
| II | Abduction Brace | 6 | 51 | 50.4 ± 11.7 | 25:26 | 12 | |||||
| Pandey, et al. [37] | 2020 | I |
Open Pouch Sling | 6 | 21 | 55.5 ± 10.5 | 9:12 | 12 | Single Row (18); Double Row (24) | pROM at 6 weeks, aaROM at 8 weeks | VAS, CMS, Vascular Flow, Healing (ultrasound) |
| Abduction Brace (30°) | 6 | 21 | 55.8 ± 7.8 | 13:8 | 12 | ||||||
| Abbreviations: SD: Standard Deviation; M:F: Male to Female; NR: Not Reported; Prom: Passive Range of Motion; aROM: Active Range of Motion; ROM: Range of Motionl; DASH: Disabilities of the Arm; Shoulder & Hand; VAS: Visual Analog Scale; SST: Simple Shoulder Test; ASES: American Shoulder & Elbow Society; CMS: Constant-Murley Score; WORC: Western Ontario Rotator Cuff | |||||||||||
Patient reported outcomes
A double-blind randomized controlled trial by Conti, et al. [32] found no significant difference in the UCLA, DASH, SST, and Constant scores between patients immobilized in an abducted and externally rotated position when compared to those immobilized in 15° of internal rotation.
Similarly, Hollman and colleagues [34] found no significant differences in function and quality of life between groups at all follow-up time points. Pandey, et al. reported no significant difference in Constant scores at 1-year follow-up between the sling and abduction brace groups in their study [37].
The study by Ghandour, et al. observed no differences in Constant-Murley scores between the abduction brace and sling groups at one year following arthroscopic rotator cuff repair [36] (Table 4).
| Table 4: Clinical measures of studies investigating sling and abduction brace after rotator cuff repair. | ||||||||||||||||||||||||
| Study | Immobilization method | Adherence to therapy | Pre-op ROM | 1y Post-op ROM | Pre-op PROMS | Final Post-op PROMS | Retear | Complications | ||||||||||||||||
| Yes:No | FF | AB | ER | IR | FF | AB | ER | IR | Constant | ASES | WORC | SST | VAS | UCLA | Constant | ASES | WORC | SST | VAS | UCLA | ||||
| Conti, et al. [32] | Internal Rotation Sling | NR | Only available in graphs | NR | NR | |||||||||||||||||||
| External Rotation + Abduction Brace | NR | Only available in graphs | NR | NR | ||||||||||||||||||||
| Silverio, et al. [33] | Abduction Brace | 88% ± 10 (59.2 - 100) | NR | NR | NR | NR | NR | NR | NR | NR | NR | 23.6 (3.3-76.7) | NR | 2.93 (0-3) | NR | 13.7 ( 5.2-25.8) | NR | 74.6 (11-95) | NR | 9 ( 2-12) | NR | 28.5 (16.5-34.5) | NR | NR |
| Hollman, et al. [34] | Anti-Rotation Sling | 15:01 | NR | 81.3 ± 12.97 | 68.7 ± 16.16 | NR | Only available in graphs * | NR | 44.2 ± 20.62 | NR | 38.5 ± 21.91 | NR | 40.9 ± 26.30 | NR | Only available in graphs^ | NR | Only available in graphs^ | NR | NR | NR | No re-tears at 3 months | 3/16 adhesive capsulitis | ||
| Abduction Brace | 17:03 | NR | 77.8 ± 15.52 | 65.9 ± 16.29 | NR | Only available in graphs * | NR | 43.4 ± 13.72 | NR | 42.1 ± 15.46 | NR | 40.6 ± 30.6 | NR | Only available in graphs^ | NR | Only available in graphs^ | NR | NR | NR | No re-tears at 3 months | 2/20 adhesive capsulitis | |||
| McColl, et al. [35] | Abduction Brace | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | NR | 15% | NR |
| Ghandour, et al. [36] | Open Pouch Sling | NR | NR | NR | NR | NR | NR | NR | NR | NR | 41.2 ± 3.4 | NR | NR | NR | 74.9 ± 12 | NR | 84.5 ± 5.7 | NR | NR | NR | 18.5 ± 4.3 | NR | NR | NR |
| Abduction Brace | NR | NR | NR | NR | NR | NR | NR | NR | NR | 40.9 ± 3.2 | NR | NR | NR | 75.6 ± 11 | NR | 84.7 ± 5.8 | NR | NR | NR | 17.7 ± 4.2 | NR | NR | NR | |
| Pandey, et al. [37] | Open Pouch Sling | NR | NR | NR | NR | NR | NR | NR | NR | NR | 30.25 (5.46) | NR | NR | NR | 8.15 /10 (1.21) | NR | 84.63 (8.33) | NR | NR | NR | 1.92 (1.44) | NR | 2/21 | NR |
| Abduction Brace | NR | NR | NR | NR | NR | NR | NR | NR | NR | 32.43 (5.22) | NR | NR | NR | 8.27 /10(1.22) | NR | 82.93 (4.16) | NR | NR | NR | 1.0 (1.0) | NR | 3/21 | NR | |
| *A significant improvement was observed in both groups in active forward elevation, glenohumeral abduction, and external rotation from 6 weeks to 3 months, from 3 to 6 months, and then 6 to 12 months after surgery (p < .001 for all analysis). ^A significant improvement was observed in both groups in the CMS and WORC index from 6 weeks to 3 months, from 3 to 6 months, and then 6 to 12 months after surgery (p < .001 for all analysis) Abbreviations: ROM: Range of Motion; PROMS: Patient Reported Outcomes; FF: Forward Flexion; AB: Abduction; ER: External Rotation; IR: Internal Rotation; ASES: American Shoulder and Elbow Score; WORC: Western Ontario Rotator Cuff; SST: Simple Shoulder Test; VAS: Visual Analogue Scale; NR: Not Reported |
||||||||||||||||||||||||
Range of motion
A double-blind randomized controlled trial by Conti, et al. [32] noted significantly greater abduction and external rotation at 1-, 3- and 6-months post-operative for patients immobilized in an abducted and externally rotated position compared to those immobilized in 15° of internal rotation (p < 0.05). Forward flexion was noted to be greater in this group at 1 month, however, no differences were noted between groups at 3- or 6 months postoperatively. On the contrary, a randomized controlled trial by Hollman, et al. demonstrated no significant differences between the anti-rotation and abduction sling groups (Table 4).
Pain
Conti and colleagues [32], found that patients immobilized in an abducted and externally rotated position had significantly less pain than those in a sling at all postoperative time points up to 6 months of follow-up (p < 0.05). On the contrary, both Hollman, et al. [34] and Ghandour, et al. found no significant difference in pain between groups at all post-operative follow-ups. Pandey and coworkers [37] reported lower VAS scores among patients in the abduction brace versus sling group, the difference approached but did not reach statistical significance (p = 0.06) (Table 4).
Re-tear rate
Two studies commented on post-operative re-tear incidence. A case series of 1600 patients by McColl, et al. [35] reported a mean re-tear rate of 15% detected by ultrasonography at 6-month follow-up. The authors found postoperative abduction sling use to be a protective factor against re-tear. Anterior-to-posterior diameter of the tear size was the greatest predictor. Less aggressive rehabilitation, abduction brace use, and increased surgical experience were associated with a significant reduction in retear rates. Conversely, a randomized controlled trial by Hollman, et al. examined the effect of tear size, surgical technique, number of anchors, amount of retraction, and intraoperative tension on outcomes in both the abduction brace and sling group and found no significant differences between the randomized groups at short term follow up of 3 months. Pandey and coworkers [37] noted a combined partial and full retear rate of 9.5% (2 of 21) among the sling group compared to 14.3% (3 of 21) in the abduction brace group. This difference in re-tear rates between the groups did not reach statistical significance (p > 0.05) (Table 4).
Biomechanical studies
A total of nine biomechanical studies were included in this review, comprising seven cadaveric studies involving 55 human shoulders (Table 1), as well as two computational shoulder models (Table 2). Zuckerman, et al. assessed strain levels after rotator cuff repair, focusing on small-sized tears (specifically supraspinatus tears) across cadaveric shoulders positioned in 36 distinct configurations [24]. Results indicated a significant increase in strain (p < 0.01) with a lower angle of abduction from 30° to 15°. A comparable pattern was demonstrated in the large tear group (involving the supraspinatus and infraspinatus tears), with pronounced strain increases observed at 15° (20N) and 0° (> 50N) of abduction.
Hatakeyama, et al. and colleagues assessed 50 distinct shoulder configurations, incorporating various degrees of elevation in the scapular, coronal, and sagittal planes, as well as arm rotation relative to the scapular plane [25]. Statistical analyses demonstrated a significant (p < 0.05) rise in rotator cuff strain with decreased humeral elevation from 30° to 15°, and from 15° to 0°, in both coronal and scapular planes. Internal rotation elicited a significant (p < 0.01) strain increase, while external rotation produced the opposite effect. Strain remained low across all degrees of rotation at 30° of elevation in the scapular plane.
Reilly, et al. evaluated gap formation after rotator cuff repair and identified 30° of abduction as an advantageous position [26]. They noted a mean reduction in passive load of 34N among shoulders abducted at 30° compared to 0°. Andarawis-Puri, et al. studied the impact of arm positioning on differential strain within the infraspinatus and supraspinatus tendons [38]. The maximal strain on the infraspinatus tendon was observed at 0° abduction compared to 30° and 60°, while maximal strain in the supraspinatus tendon occurred at 60° and minimal strain at 30° of abduction. The authors also observed the greatest mechanical interaction between the infraspinatus and supraspinatus at 0° of abduction and the lowest at 30°, suggesting 30° of abduction as the optimal immobilization position post-rotator cuff repair to minimize strain on the repair.
Park, et al. investigated footprint contact area and pressure in human cadaveric models with full-thickness supraspinatus tears [38]. They found that the highest contact area and pressure occurred at 0° of abduction and the lowest at 60°, with no significant difference in contact area observed between abduction angles of 0° to 30°. Internal rotation was favored for contact area and pressure compared to external rotation.
Hawthorne, et al. observed that glenohumeral joint abduction of 4° was seen with a traditional sling. A small abduction pillow translated to 22° of internal rotation and 13° of glenohumeral joint abduction, while a large abduction pillow translated 11° and 25° of glenohumeral joint abduction respectively. Lower levels of anterior and posterior tendon strain were seen with increasing abduction angles from 0 to 25° (p < 0.001). The use of a small abduction pillow reduced tension on the supraspinatus by 27% anteriorly and 55% posteriorly, while a large abduction pillow led to a further reduction in tension to 42% and 56% respectively.
Howe, et al. conducted a cadaveric study, finding that external rotation of 30° resulted in ten times greater tension in the anterior suture compared to the posterior suture (p < 0.001), with the opposite observed during internal rotation [28]. The authors recommended neutral rotation as it may minimize tension at all suture locations, providing a safer shoulder immobilization position post-rotator cuff repair.
Saul, et al. conducted a simulation analysis investigating the passive tension and moment-generating capacity of the supraspinatus muscle under varying gap lengths and shoulder positions [31]. They observed that passive force increased significantly from 29N to 518N as the shoulder moved from 60° to 0° of abduction, surpassing the previously reported pull-out strength value of 215N [24,25]. Their findings suggested that the optimal shoulder posture, particularly for minimizing strain on the supraspinatus and infraspinatus tendons, was approximately 30° of abduction with neutral rotation. Jackson, et al. similarly noted this trend, suggesting potential adjustments in elevation depending on the specific rotator cuff tendon involved [30]. Their computational model analyzed the ideal position of the glenohumeral joint and demonstrated that strains at the repair site for isolated supraspinatus tears could be reduced by 76% to 90% by utilizing an abduction pillow compared to having an arm at the side.
Overall, numerous biomechanical studies demonstrate glenohumeral joint abduction to be protective for rotator cuff repairs in a relatively dose-dependent manner, with the majority of studies favoring 30° of abduction as the optimal position. Biomechanical data shows abduction in the coronal and scapular planes to be protective in minimizing strain, as well as gap formation while improving contact area and pressure on the repair [24,26]. The rotational profile of the arm post-operatively appeared to have significant effects on rotator cuff strain as well as contact area and pressure at the repair site as well [29,38]. Increasing internal rotation led to greater tension in the posterior rotator cuff and greater external rotation led to greater tension in the anterior rotator cuff.
A large abduction pillow which clinically translates to glenohumeral abduction of 25° and internal rotation of 11°, showed a reduction in supraspinatous tension by 42% anteriorly and 56% posteriorly, compared with a traditional sling [29]. Biomechanically, studies overall demonstrated that an abduction pillow which increases the angle of abduction in the scapular plane and decreases internal rotation of the arm is a safer environment for the rotator cuff to heal. Despite the strong evidence seen in biomechanical studies, it did not translate to superiority in clinical outcomes for abduction brace compared with traditional sling.
Overall, our literature search demonstrated a dearth of studies comparing clinical outcomes of various immobilization positions in patients undergoing rotator cuff repair. In the current systematic review, immobilization with an abduction brace did not lead to convincing improvements in ROM, and pain, patients reported outcomes such as ASES, UCLA, SST scores, or re-tear rates over sling immobilization.
A double-blinded randomized controlled trial by Conti et al, which evaluated 40 total patients undergoing repair of isolated superior or posterosuperior rotator cuff tears demonstrated the most favorable results in favor of those immobilized with an abduction brace. In those immobilized with an abduction brace, better active glenohumeral abduction, and external rotation were demonstrated at all time points including their final follow-up at 6 months, while demonstrating lower VAS pain scores at all time points.
However, even in this study, they ultimately found no significant difference in the UCLA, DASH, SST, and Constant-Murley scores between the abduction brace and traditional sling group [32]. Other clinical studies included in this review, including two level-I randomized controlled trials [34,37], as well as two level-II prospective cohort studies [33,36], and a level-III retrospective cohort study [35] essentially failed to find the superiority of abduction brace over traditional sling in all outcomes measured. Interestingly, Pandey et al, found ultrasonographic evidence of increased blood flow in the repair at 6 weeks post-operatively which did not translate to any superior clinical outcomes [37].
There are a variety of factors that may account for the discrepancy between the biomechanical and clinical findings reported in the current review. One such factor is compliance with the method of immobilization. While it is well known from other areas of the orthopedic literature that patient adherence to bracing and immobilization is low [39-43], compliance with the wear time of abduction braces has been identified to be very unreliably reported [33,34,41]. In 2018, Grubhofer studied abduction brace compliance rates in 50 post-operative patients by utilizing a temperature sensor implanted into their braces, they found a statistically significant (p < 0.001) discrepancy of 21% between self-reported and objectively measured rates [41]. Decreased compliance to both abduction brace and traditional sling in clinical studies would make it difficult to reliably assess the effects of either treatment in a clinical study. Only two clinical studies in this review evaluated the compliance rate of their immobilization method in a self-reported manner [33,34].
The significant findings seen in biomechanical studies truly do not translate to differences significant enough to meet the minimal threshold to be clinically relevant regarding patient outcomes such as pain, PROM, ROM, and re-tear rates after rotator cuff repair. For instance, Pandey et al found ultrasonographic evidence of increased blood flow in the repair at 6 weeks post-operatively with the utilization of abduction bracing, but it did not translate to any superior clinical outcomes [37]. The glenohumeral joint is an incredibly complex joint with soft tissue interactions between various peri-scapular muscles. Strain levels and differential levels in contact pressure, area, and gap formation seen in biomechanical studies may therefore be less relevant in a complex dynamic model that exactly mimics the clinical shoulder after a rotator cuff repair.
Limitations of this study are as follows: Firstly, there was significant heterogeneity in the tear characteristics, surgical techniques, and abduction braces (including the angle of abduction) used by the included clinical studies. Secondly, McColl, et al., not with standing, the eligible clinical studies consisted of small sample sizes. Thirdly, the heterogeneity among outcomes reported by the clinical studies limited our ability to quantitatively pool the results. Another limitation is non-uniform rehabilitation protocols among the studies included. All studies allowed immediate pendulum motion, with active ROM beginning at the latest 6 weeks post-operatively. One study utilized a more accelerated rehabilitation protocol with an active range of motion starting at day 8, progressing to a more conservative rehabilitation protocol as the study progressed [35]. The slight variations in rehabilitation protocols could have affected clinical outcomes especially post-operative pain levels as early ROM. Despite these limitations, the present study provides a comprehensive review of the current state of the literature on the effect of postoperative immobilization position on outcomes following arthroscopic rotator cuff repair. Future prospective studies with a large sample size and uniform rehabilitation protocols are needed to investigate the effect of immobilization position among patients with similar rotator cuff tear sizes, with longer radiographic and clinical evaluations.
Based on current biomechanical evidence, placement of the arm into an abducted position following rotator cuff repair was found to be favorable. An abduction angle of 30° was associated with lower strain on the repair while maintaining appropriate contact pressure at the footprint. However, the use of an abduction brace did not result in a clinically significant improvement in PROM, ROM, and re-tear rates when compared to a traditional sling in clinical studies. Future studies with a greater sample size are needed to prospectively investigate the effect of immobilization position among patients with similar rotator cuff tear sizes and with longer radiographic and clinical re-evaluations.
- Largacha M, Parsons IM, Campbell B, Titelman RM, Smith KL, Matsen F 3rd. Deficits in shoulder function and general health associated with sixteen common shoulder diagnoses: a study of 2674 patients. J Shoulder Elbow Surg. 2006;15:30-39. Available from: https://doi.org/10.1016/j.jse.2005.04.006
- Flatow EL, Soslowsky LJ, Ticker JB, Pawluk RJ, Hepler M, Ark J, et al. Excursion of the rotator cuff under the acromion. Patterns of subacromial contact. Am J Sports Med. 1994;22:779-788. Available from: https://doi.org/10.1177/036354659402200609
- Yamamoto A, Takagishi K, Osawa T, Yanagawa T, Nakajima D, Shitara H, Prevalence and risk factors of a rotator cuff tear in the general population. J Shoulder Elbow Surg. 2010;19:116-120. Available from: https://doi.org/10.1016/j.jse.2009.04.006
- Tempelhof S, Rupp S, Seil R. Age-related prevalence of rotator cuff tears in asymptomatic shoulders. J Shoulder Elbow Surg. 1999;8:296-299. Available from: https://doi.org/10.1016/s1058-2746(99)90148-9
- Chang KV, Hung CY, Han DS, Chen WS, Wang TG, Chien KL. Early versus delayed passive range of motion exercise for arthroscopic rotator cuff repair: a meta-analysis of randomized controlled trials. Am J Sports Med. 2015;43:1265-1273. Available from: https://doi.org/10.1177/0363546514544698
- Kim YS, Chung SW, Kim JY, Ok JH, Park I, Oh JH. Is early passive motion exercise necessary after arthroscopic rotator cuff repair? Am J Sports Med. 2012;40:815-21. Available from: https://doi.org/10.1177/0363546511434287
- Keener JD, Galatz LM, Stobbs-Cucchi G, Patton R, Yamaguchi K. Rehabilitation following arthroscopic rotator cuff repair: a prospective randomized trial of immobilization compared with early motion. J Bone Joint Surg Am. 2014;96:11-19. Available from: https://doi.org/10.2106/jbjs.m.00034
- Tashjian RZ, Hollins AM, Kim HM, Teefey SA, Middleton WD, Steger-May K, et al. Factors affecting healing rates after arthroscopic double-row rotator cuff repair. Am J Sports Med. 2010;38:2435-2442. Available from: https://doi.org/10.1177/0363546510382835
- Slabaugh MA, Nho SJ, Grumet RC, Wilson JB, Seroyer ST, Frank RM, et al. Does the literature confirm superior clinical results in radiographically healed rotator cuffs after rotator cuff repair? Arthroscopy. 2010;26:393-403. Available from: https://doi.org/10.1016/j.arthro.2009.07.023
- Galatz LM, Ball CM, Teefey SA, Middleton WD, Yamaguchi K. The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears. J Bone Joint Surg Am. 2004;86:219-224. Available from: https://doi.org/10.2106/00004623-200402000-00002
- Riboh JC, Garrigues GE. Early passive motion versus immobilization after arthroscopic rotator cuff repair. Arthroscopy. 2014;30:997-1005. Available from: https://doi.org/10.1016/j.arthro.2014.03.012
- Thomopoulos S, Williams GR, Soslowsky LJ. Tendon to bone healing: differences in biomechanical, structural, and compositional properties due to a range of activity levels. J Biomech Eng. 2003;125:106-113. Available from: https://doi.org/10.1115/1.1536660
- Sonnabend DH, Howlett CR, Young AA. Histological evaluation of repair of the rotator cuff in a primate model. J Bone Joint Surg Br. 2010;92:586-594. Available from: https://doi.org/10.1302/0301-620x.92b4.22371
- Parsons BO, Gruson KI, Chen DD, Harrison AK, Gladstone J, Flatow EL. Does slower rehabilitation after arthroscopic rotator cuff repair lead to long-term stiffness? J Shoulder Elbow Surg. 2010;19:1034-1039. Available from: https://doi.org/10.1016/j.jse.2010.04.006
- Sheps DM, Silveira A, Beaupre L, Styles-Tripp F, Balyk R, Lalani A, Glasgow R, et al. Early active motion versus sling immobilization after arthroscopic rotator cuff repair: a randomized controlled trial. Arthroscopy. 2019;35:749-60.e2. Available from: https://doi.org/10.1016/j.arthro.2018.10.139
- Arndt J, Clavert P, Mielcarek P, Bouchaib J, Meyer N, Kempf JF. Immediate passive motion versus immobilization after endoscopic supraspinatus tendon repair: a prospective randomized study. Orthop Traumatol Surg Res. 2012;98. Available from: https://doi.org/10.1016/j.otsr.2012.05.003
- Jenssen KK, Lundgreen K, Madsen JE, Kvakestad R, Pripp AH, Dimmen S. No functional difference between three and six weeks of immobilization after arthroscopic rotator cuff repair: a prospective randomized controlled non-inferiority trial. Arthroscopy. 2018;34:2765-2774. Available from: https://doi.org/10.1016/j.arthro.2018.05.036
- Tirefort J, Schwitzguebel AJ, Collin P, Nowak A, Plomb-Holmes C, Lädermann A. Postoperative mobilization after superior rotator cuff repair: sling versus no sling: a randomized prospective study. J Bone Joint Surg Am. 2019;101:494-503. Available from: https://doi.org/10.2106/jbjs.18.00773
- Cuff DJ, Pupello DR. Prospective randomized study of arthroscopic rotator cuff repair using an early versus delayed postoperative physical therapy protocol. J Shoulder Elbow Surg. 2012;21:1450-1455. Available from: https://doi.org/10.1016/j.jse.2012.01.025
- Lee BG, Cho NS, Rhee YG. Effect of two rehabilitation protocols on range of motion and healing rates after arthroscopic rotator cuff repair: aggressive versus limited early passive exercises. Arthroscopy. 2012;28:34-42. Available from: https://doi.org/10.1016/j.arthro.2011.07.012
- Pedowitz RA, Yamaguchi K, Ahmad CS, Burks RT, Flatow EL, Green A, et al. Optimizing the management of rotator cuff problems. J Am Acad Orthop Surg. 2011;19:368-379. Available from: https://doi.org/10.5435/00124635-201106000-00007
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339. Available from: https://doi.org/10.1371/journal.pmed.1000097
- Slim K, Nini E, Forestier D, Panis Y, Chipponi J. Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ J Surg. 2003;73:712-716. Available from: https://doi.org/10.1046/j.1445-2197.2003.02748.x
- Zuckerman JD, Leblanc JM, Choueka J, Kummer F. The effect of arm position and capsular release on rotator cuff repair: a biomechanical study. J Bone Joint Surg Br. 1991;73:402-405. Available from: https://doi.org/10.1302/0301-620x.73b3.1670437
- Hatakeyama Y, Itoi E, Pradhan RL, Urayama M, Sato K. Effect of arm elevation and rotation on the strain in the repaired rotator cuff tendon: a cadaveric study. Am J Sports Med. 2001;29:788-794. Available from: https://doi.org/10.1177/03635465010290061901
- Reilly P, Bull AM, Amis AA, Wallace AL, Richards A, Hill AM, et al. Passive tension and gap formation of rotator cuff repairs. J Shoulder Elbow Surg. 2004;13:664-667. Available from: https://doi.org/10.1016/j.jse.2004.03.011
- Andarawis-Puri N, Kuntz AF, Ramsey ML, Soslowsky LJ. Effect of glenohumeral abduction angle on the mechanical interaction between the supraspinatus and infraspinatus tendons for the intact, partial-thickness torn, and repaired supraspinatus tendon conditions. J Orthop Res. 2010;28:846-851. Available from: https://doi.org/10.1002/jor.21068
- Howe C, Huber P, Wolf FM, Matsen F 3rd. Differential suture loading in an experimental rotator cuff repair. Am J Sports Med. 2009;37:324-329. Available from: https://doi.org/10.1177/0363546508324308
- Hawthorne JR, Carpenter EM, Lam PH, Murrell GAC. Effects of abduction pillows on rotator cuff repair: a biomechanical analysis. HSS J. 2018;14:114-122. Available from: https://doi.org/10.1007/s11420-017-9592-2
- Jackson M, Tétreault P, Allard P, Begon M. Optimal shoulder immobilization postures following surgical repair of rotator cuff tears: a simulation analysis. J Shoulder Elbow Surg. 2013;22:1011-1018. Available from: https://doi.org/10.1016/j.jse.2012.10.042
- Saul KR, Hayon S, Smith TL, Tuohy CJ, Mannava S. Postural dependence of passive tension in the supraspinatus following rotator cuff repair: a simulation analysis. Clin Biomech (Bristol, Avon). 2011;26:804-810. Available from: https://doi.org/10.1016/j.clinbiomech.2011.04.005
- Conti M, Garofalo R, Castagna A. Does a brace influence clinical outcomes after arthroscopic rotator cuff repair? Musculoskelet Surg. 2015;99 Suppl 1. Available from: https://doi.org/10.1007/s12306-015-0357-0
- Silverio LM, Cheung EV. Patient adherence with postoperative restrictions after rotator cuff repair. J Shoulder Elbow Surg. 2014;23:508-513. Available from: https://doi.org/10.1016/j.jse.2013.09.018
- Hollman F, Wolterbeek N, Zijl JAC, van Egeraat SPM, Wessel RN. Abduction brace versus antirotation sling after arthroscopic cuff repair: the effects on pain and function. Arthroscopy. 2017;33:1618-1626. Available from: https://doi.org/10.1016/j.arthro.2017.02.010
- McColl AH, Lam PH, Murrell GAC. Are we getting any better? A study on repair integrity in 1600 consecutive arthroscopic rotator cuff repairs. JSES Open Access. 2019;3:12-20. Available from: https://doi.org/10.1016%2Fj.jses.2019.01.002
- Ghandour TM, Ibrahim A, Abdelrahman AA, Elgammal A, Hammad MH. Does the type of shoulder brace affect postoperative pain and clinical outcome after arthroscopic rotator cuff repair? Arthroscopy. 2019;35:1016-1023. Available from: https://doi.org/10.1016/j.arthro.2018.10.137
- Pandey V, Madi S, Maddukuri S, Acharya K, Karegowda LH, Willems WJ. Does application of abduction brace after arthroscopic rotator cuff repair improve blood flow around posterosuperior rotator cuff and repair site, affecting pain levels and clinical and structural outcomes? A pilot randomized controlled trial. JSES Int. 2020;4:848-859. Available from: https://doi.org/10.1016%2Fj.jseint.2020.07.021
- Park MC, Pirolo JM, Park CJ, Tibone JE, McGarry MH, Lee TQ. The effect of abduction and rotation on footprint contact for single-row, double-row, and modified double-row rotator cuff repair techniques. Am J Sports Med. 2009;37:1599-608. Available from: https://doi.org/10.1177/0363546509332506
- Morton A, Riddle R, Buchanan R, Katz D, Birch J. Accuracy in the prediction and estimation of adherence to bracewear before and during treatment of adolescent idiopathic scoliosis. J Pediatr Orthop. 2008;28:336-341. Available from: https://doi.org/10.1097/bpo.0b013e318168d154
- Duivenvoorden T, van Raaij TM, Horemans HL, Brouwer RW, Bos PK, Bierma-Zeinstra SM, et al. Do laterally wedged insoles or valgus braces unload the medial compartment of the knee in patients with osteoarthritis? Clin Orthop Relat Res. 2015;473:265-274. Available from: https://doi.org/10.1007%2Fs11999-014-3947-5
- Grubhofer F, Catanzaro S, Schöpbach R, Imam MA, Wirth S. Compressive stockings after hindfoot and ankle surgery. Foot Ankle Int. 2018;39:210-218. Available from: https://doi.org/10.1177/1071100717737518
- Takemitsu M, Bowen JR, Rahman T, Glutting JJ, Scott CB. Compliance monitoring of brace treatment for patients with idiopathic scoliosis. Spine (Phila Pa 1976). 2004;29:2070-2074; discussion 2074. Available from: https://doi.org/10.1097/01.brs.0000138280.43663.7b
- Raju S, Lurie F, O’Donnell TF. Compression use in the era of endovenous interventions and wound care centers. J Vasc Surg Venous Lymphat Disord. 2016;4:346-354. Available from: https://doi.org/10.1016/j.jvsv.2015.11.001