
More Information
Submitted: September 13, 2023 | Approved: April 29, 2024 | Published: April 30, 2024
How to cite this article: Gaspar AP, De Matos LDNJ, Amorim S, De Oliveira RS, Fernandes RV, et al. The Comparison of Brachial Artery Parameters between the Clinical Cuff, Pneumatic Controlled Air Band (KAATSU), and Elastic Band during Blood Flow Restriction at the same Perceived Tightness. J Sports Med Ther. 2024; 9: 015-021.
DOI: 10.29328/journal.jsmt.1001076
Copyright License: © 2024 Gaspar AP, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Blood flow restriction; KAATSU; Perceived tightness; Sphygmomanometer cuff; Practical blood flow restriction

The Comparison of Brachial Artery Parameters between the Clinical Cuff, Pneumatic Controlled Air Band (KAATSU), and Elastic Band during Blood Flow Restriction at the same Perceived Tightness
Alexandra Passos Gaspar1* , De Matos LDNJ1, Amorim S1, De Oliveira RS2, Fernandes RV2 and Laurentino G2
, De Matos LDNJ1, Amorim S1, De Oliveira RS2, Fernandes RV2 and Laurentino G2
1Hospital Israelita Albert Einstein, São Paulo, Brazil
2Blood Flow Restriction and Exercise Research Group, São Judas Tadeu University, SP, Brazil
*Address for Correspondence: Alexandra Passos Gaspar, PhD, Hospital Israelita Albert Einstein Avenida Albert Einstein 627, Bloco D, 3 Andar São Paulo, 05651901 Brazil, Email: [email protected]; [email protected]
The Blood Flow Restriction (BFR) technique is based on cuffs connected to a pressure device that induces partial arterial inflow. BFR combined with exercise has already been proven to increase strength, muscle mass, and muscular endurance. However, some BFR devices with pneumatic air bands, such as KAATSU (KA), are expensive and less accessible, making either a Sphygmomanometer Cuff (SC) or Elastic Band (EB) an interesting alternative. However, vascular parameters in response to blood flow restriction during KA, EB, and SC have not yet been compared.
Purpose: The aim of this study was to compare the brachial blood flow behavior during restriction using bands such as KA, SC, and EB on the same perceived tightness.
Methods: Thirty healthy men participated in a prospective crossover study. Participants underwent blood flow measurements before and during KA, SC, and EB use, with KA-perceived tightness taken as a reference. The brachial blood flow volume, the diameter of the artery, and blood flow velocity were measured before and immediately after the cuff’s inflation at a specific tightness.
Results: Blood flow volume was significantly reduced in KA (52%, ES: 1.38), SC (61.7%, ES: 1.29), and EB (41.5%, ES: 1.22) (p <.0001). In addition, blood flow velocity was significantly reduced in KA (12.9%, ES: 0.74), SC (23.8%, ES: 1.02), and EB (25.6%, ES: 1.02) (p <.0001). No significant changes were observed in the diameter of the brachial artery for any condition (p > 0.05).
Conclusion: Brachial blood flow behavior was similar between pneumatic controlled air band (KA), SC, and EB cuffs at the same perceived tightness.
Highlights
- Growing evidence suggests that blood flow restriction is an interesting technique to improve muscle mass and strength with less articular impact and practical applications are yet to be explored.
- Different bands and devices have been used to apply in patients the technique and but, methods are still too heterogenous to be compared in the expected results.
- Although studies in the BFR literature have shown that blood flow restriction is applied according to Arterial Occlusion Pressure (AOP) and the devices and techniques are trying to standardize it, there is still a lack of information on this matter. More studies are needed to evaluate their similarity and also understand their safety
The blood flow restriction technique utilizes a pneumatic cuff connected to a pressure device that proximally restricts the blood flow for the upper and/or lower limbs [1]. The KAATSU (KA) pneumatic controlled air band is one of the most commonly used devices to restrict arterial and venous blood flow and was first created and developed in Japan by Dr. Yoshiaki Sato in the middle sixties [1].
Although many different pneumatic cuff devices have been used for restricting blood flow, such as KAATSU, Vasper [2], Delfi [3], ATS 4000 [4] and Hokanson [6], in general, these devices require a high financial investment for acquisition, with some of them also demanding certification and expertise from specialists to handle the equipment. These conditions may hinder the process of acquiring equipment and implementing the BFR technique in hospitals and rehabilitation centers with fewer economic resources.
One of the most important advantages of using pneumatic controlled air bands for restricting blood flow is the maintenance of restriction pressure during all phases of the restrictive stimulus and/or during exercise performance. This partial arterial restriction, while the occlusion of venous outflow, is an advantage of the technique [6] once it prevents the risk of ischemia-induced adverse events [6].
The sphygmomanometer/pneumatic cuff (SC), also called the clinical cuff, is another device commonly used for restricting blood flow at rest or during exercise protocols [7]. Many studies have shown the use of SC with arbitrary or absolute pressure [8-11]. However, when individualized pressure is required to perform the BFR protocols with SC, in general, a handheld Doppler is needed, making the SC technique neither practical nor accessible for most practitioners.
Faced with this problem, the use of elastic bands (EB), also referred to in some studies as “practical blood flow restriction” [12,13], has been proposed as an alternative method for restricting arterial blood flow because of its accessibility and relative cost-effectiveness.
The EB technique consists of blood flow restriction using an elastic band wrapped proximally to either the participant´s thigh or arm, based on the individual´s perception of tightness. Wilson, et al. [12] reported that for all participants at perceived tightness 7 out of 10 presented femoral arterial blood flow. EB has been shown to be an effective technique to induce muscle adaptations when compared to conventional resistance training [14], but it is still unknown whether blood flow responses with the use of EB differ from other methods, such as pneumatically controlled air bands such as KAATSU and pneumatic cuff (SC), regarding vascular parameters. EB might be an alternative with low cost that is more accessible in clinical practice.
Although studies in the BFR literature have shown that blood flow restriction is applied according to Arterial Occlusion Pressure (AOP) and the devices and techniques are trying to standardize it, there is still a lack of information on this matter. There might be differences when different cuffs or pressure control devices are used (including vascular parameters) that could affect the AOP.
Therefore, the aim of this study was to compare brachial blood flow response during restriction stimulus using pneumatically controlled air bands (KAATSU), Sphygmomanometer Cuff (SC), and an Elastic Band (EB) at the same individual´s perception tightness [12]. We hypothesized that vascular parameters in response to KA, SC, and EB would be similar.
The present study used a prospective randomized crossover design in healthy physically active males recruited from São Judas Tadeu University and Israelita Albert Einstein Hospital. The sample size calculation of 30 individuals was based on a previous study conducted on healthy individuals who compared different types of cuffs [15], assuming statistical power (α = 0.05, and 1-β = 0.95) with an effect size of 0.8 and a drop out of ~20% (G* power – 3.1).
The inclusion criteria for participation assessed via medical screening were physically active men aged 18 and 45 years old. Exclusion criteria included (1) infectious disease within the last six months prior to the study; (2) smoking within the last 6 months; (3) history of anemia, cerebrovascular disease, or myocardial infarction in the last 6 months; (4) previous deep venous thrombosis; (5) use of oral anticoagulants; and (6) history of antiphospholipid syndrome. All participants were informed about the risks and benefits of this study and submitted their written informed consent prior to participation. This study was conducted according to the Declaration of Helsinki, and The Institutional Review Board (ethical committee number SGPP no. 3982-19) approved the experimental protocol.
Study design
Participants attended the laboratory for three visits. In the first two visits, participants were familiarized with the blood flow restriction techniques using KAATSU (KA), sphygmomanometer/pneumatic cuff (SC), and elastic bands (EB), and their perception of perceived tightness was taken in accordance with the scale proposed by Wilson, et al. [12]. Moreover, in familiarization sessions, brachial blood flow at rest and perceived tightness (PT) were assessed. Brachial blood flow and PT from day 1 and day 2 were used for test-retest reliability.
At the third visit, participants underwent brachial blood flow measurements with KA, SC, and EB techniques in randomized order, with 15-minute intervals between measurements. Perceived tightness on the scale (0 out of 10) was first set with KA and reproduced for both SC and EB techniques. Brachial blood flow was assessed before and during the application of each technique (Figure 1).
Flow diagram of the study with three different cuffs Measure of perceived tightness (Figure 1).
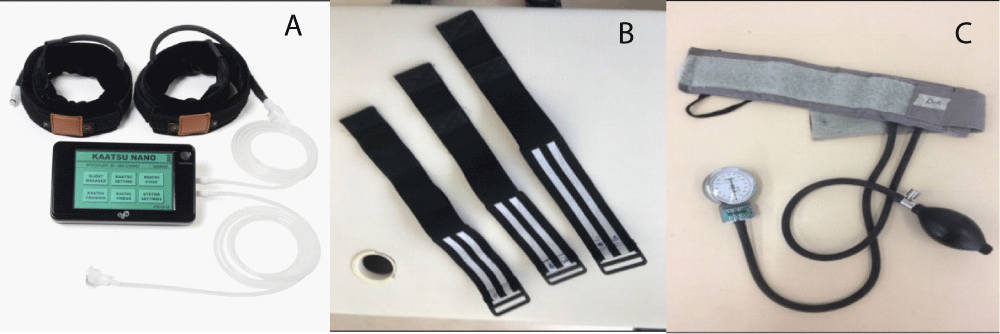
Figure 1: Blood flow restriction (BFR) technique devices. Kaatsu Nano (A), elastic band (B), and sphygmomanometer cuff (C).
The measure of perceived tightness (PT) was used to evaluate blood flow during restriction using KA, SC, and EB through a perceived tightness scale previously proposed by Wilson, et al. [12]. Participants were asked to answer the perceived tightness on a scale categorized as no tightness when perceived tightness was “0 out of 10”, moderate tightness was “7 out of 10”, and intense tightness was “10 out of 10”. Recent studies have shown that PT is a feasible method for practical application in investigations with blood flow restriction either at rest or exercises, as well as its use in rehabilitation procedures in hospitals, clinics, and home-based exercise [16,17].
Brachial blood flow measurement at rest
Blood flow measurements were assessed with the different cuffs according to recent recommendations [18]. Brachial artery images were recorded by a 2-dimensional ultrasonography device with a spectral Doppler and linear transducer (L5-12/60, Logic E (R7), GE Medical Systems, China, CO. LTD) described previously by Mouser, et al. 2017 with each participant´s right arm supported at heart level, in flexed and abduction, while participants were maintained in a seated position. Following the application of transmission gel, a wide-band linear array ultrasound probe was used to locate the brachial artery. The Doppler transducer (L5-12/60) in B pulse mode was placed on the anteromedial aspect of the arm, perpendicular to the axis of the arm, 2-10 cm proximal to the antecubital fold over the artery, and ultrasound parameters were set to optimal image acquisition. The angle of insonation was set at ≤60°.
Blood flow velocity spectra were recorded simultaneously in the 10-MHz linear pulse mode. The diameter of the artery, blood flow at rest, and blood velocity measurements were recorded continuously over 15 seconds. After the baseline recording, a cuff on the forearm was slowly inflated (for KA and SC), while the elastic band was tightened according to the perceived tightness from KA Optimal Pressure (KOP) for each participant´s arm. Following blood flow measurements, the probe was removed, the cuffs were deflated, and the tightness of EB was released. All measurements were taken in a single day in random order.
For each blood flow measurement, the end-diastolic diameter of the lumen of the brachial artery was measured using on-screen calipers, and blood flow was calculated using manufacturer-provided software (Logic E, (R7), GE Medical Systems, China, CO. LTD). Blood flow volume (ml/min) and blood flow velocity (cm/sec) data were recorded across 15 s, and data from the last ten consecutive cardiac cycles were recorded and averaged for each measurement. All measures were performed offline and by the same researcher.
Measurement of brachial arterial blood flow with KAATSU
After participants had rested for 15 minutes in a seated position, a KAATSU (KA) cuff (5 cm wide) was applied to the most proximal portion of the participant´s right arm. The pneumatic cuff was connected to the device (KAATSU Nano model, KAATSU Global Inc. Japan). The cuff was inflated to determine KA base pressure (KBP), and increments of pressure of 10 standard KAATSU units (SKU) every 5-10 s were performed until ~20 to 25 SKU, following the manufacturer´s instructions [1]. After KBP was attained, additional increments of pressure were performed on the KA device to determine the KA Optimum Pressure (KOP). During KBP and KA optimum pressure measurements, participants were asked to rate the perceived tightness in KA across 5-10 s to each increment of pressure, following the procedures used by Wilson, et al. [12]. After perceived tightness at KA, optimum pressure was determined, the KA cuff was deflated and removed, and then the participants rested for 5 min before starting blood flow measurements.
The perceived tightness obtained during KOP was taken as a reference for blood flow measurements with EB and SC. Blood flow measurements were assessed on the same day, with a 15-minute interval minutes between them.
It has been reported that a pressure gauge was used to establish a conversion from SKU to mmHg, and it was found that 1 SKU is equal to 1 mmHg [19]. The correct KA optimal pressure is, first, not so high as to occlude blood flow and, second, high enough to achieve a profound “disturbance of homeostasis”. In addition, the participants should always have a present capillary refill and feel pulsation under the air bands [1].
Measurement of brachial arterial flow with sphygmomanometer/pneumatic cuff
A baseline blood flow measurement, arterial pressure (AOP), and perceived tightness in KAATSU optimum pressure were determined using a sphygmomanometer/pneumatic cuff. A sphygmomanometer/pneumatic cuff (SC), nylon material (6 cm wide and 35 cm long) was positioned on the most proximal region of the participant´s dominant arm.
Using a portable Doppler device probe (DV-600) positioned on the radial artery of the participants, the cuff was then inflated at the lowest pressure until the auscultatory arterial pulse was no longer detected. This point was considered as AOP (184.6 ± 41.7 mmHg), and then, the cuff was deflated. Next, an initial pressure of ~40 mmHg, followed by cycles of 5 to 10 mmHg, was conducted in SC until the participants reported a similar perceived tightness value recorded in KA optimal pressure, with each increment cycle lasting a period of ~5-10 s. After participants had identified the PT in SC, the restriction pressure was recorded (101.9 ± 37.2 mmHg), and the cuff was deflated. After 5 min of rest, brachial blood flow measurement was evaluated during a 15s period.
Measurement of brachial arterial flow with the elastic band technique
A baseline blood flow measurement, perceived tightness (PT) in KAATSU Optimum Pressure (KOP), was taken from each participant´s arm to match PT to be used during the blood flow restriction measurement with an elastic band. After 5 min of rest, an elastic band (6 cm wide and 53 cm length) was positioned on the proximal region of the dominant arm, and then, the elastic band was tightened with increments of ~1 to 2 cm, with cycles of tightness of ~5-10 s, until the participants reported the level of PT recorded in KOP. The tightness of the elastic band was released, and after 5 min of rest, brachial blood flow was measured during a 15s period.
Statistical analysis
Initially, data normality was tested by the Shapiro‒Wilk test. Data are presented as normal distributions for brachial artery diameter and peak velocity through parametric statistical tests. For comparison between protocols, the mixed model for repeated measurements was applied as a fixed factor (KA, SC cuff, and EB and time (baseline and during KOP)).
For brachial artery blood flow, as data were not found to be normal by the Shapiro‒Wilk test, a nonparametric test, and Friedman’s test were chosen for data analysis. In the presence of significant F, Tukey’s post hoc test was used to identify the differences between the protocols. We also calculated the effect size (ES), a magnitude-based analysis between moments (Nakagawa and Cuthill 2007), as follows: ES = meanpost – meanpre/√(Npre-1)SD2 + (Npost-1)SD2/Npre + Npost. Statistical significance was set at p£ 0.05. Data were analyzed using the Statistical Package SPSS (IBM SPSS Statistics for Windows, Version 24.0, 2016).
The participants’ characteristics of the study are described in Table 1.
| Table 1: Participant characteristics for the total sample (N = 30). | |
| Variables | Mean (SD) |
| Age (years) | 33.8 ± 8.5 |
| Body mass (kg) | 82.5 ± 14.9 |
| Height (m) | 1.75 ± 0.1 |
| BMI (kg/m2) | 26.9 ± 3.7 |
| Arm circumference (cm) | 33.1 ± 4.1 |
| Arm AOP (mmHg) | 184.6 ± 41.7 |
| SD: Standard Deviation; BMI: Body Mass Index; AOP: Arterial Occlusion Pressure. | |
An initial analysis revealed no differences between conditions in baseline values for all dependent variables (p > 0.05). The mean perceived tightness (PT) in KAATSU Optimal Pressure (KOP) and SC was 4.2 ± 2.0, while in EB, it was 4.3 ± 2.1 based on a perceived tightness scale from 0 out of 10 [12].
The restriction pressure recorded in SC was 101.9 ± 37.2 mmHg, which meant ~ 55.3% of the participant´s Arterial Occlusion Pressure (AOP) at the KAATSU Optimal Pressure (KOP), according to individual perceived tightness. None of the participants were detected to have total arterial occlusion during KA, SC, or EB.
Table 2 summarizes Blood flow volume, blood flow velocity, and diameter of the brachial artery before and after KAATSU, the Elastic Band (EB), and the Sphygmomanometer Cuff (SC).
| Table 2: Blood flow volume, blood flow velocity, and diameter ofthe brachial artery before and after KAATSU, the elastic band (EB), and thesphygmomanometer cuff (SC). | ||||
| Variables | Baseline | KAATSU | EB | SC |
| Mean ± (SD) | Mean ± (SD) | Mean ± (SD) | ||
| Blood flow volume (ml/min) | 127.2 ± 69.9 | 51.9 ± 32.3 | 56.6 ± 46.8 | 54.7 ± 37.1 |
| % Change | ------- | 59.1 | 55.5 | 57.0 |
| Baseline | KAATSU | EB | SC | |
| Blood flow velocity(cm/s) | 75.8 ± 16.4 | 63.0 ± 17.9 | 53.4 ± 15.8 | 59.1 ± 16.2 |
| %Change | ------- | 16.0 | 22.0 | 21.6 |
| Baseline | KAATSU | EB | SC | |
| Diameter of artery(cm) | 0.46 ± 0.05 | 0.46 ± 0.05 | 0.45 ± 0.06 | 0.45 ± 0.05 |
| %Change | 0 | 2.1 | 2.1 | |
Blood flow volume at rest
There was a significant time effect for blood flow (p < 0.0001) with no interaction condition*time (p = 0.632). Blood flow was significantly reduced in the KA (52%, ES: 1.38, CI: 34.8 – 69.0 ml/min, p < .0001), SC (61.7%, ES: 1.29, CI: 37.6 – 71.9 ml/min, p < .0001), and EB (41.5%, ES: 1.22, CI: 39.5 – 73.7 ml/min, p < .0001) groups (Figure 2). No significant difference was observed between conditions (p > 0.05). Test-retest reliability of blood flow volume using standard error of measurement (SEM), the minimal difference needed to be considered real (MD), and coefficient of variation (CV%) were 36.7 ml/min, 101.8 ml/min, and 4.9%, respectively.
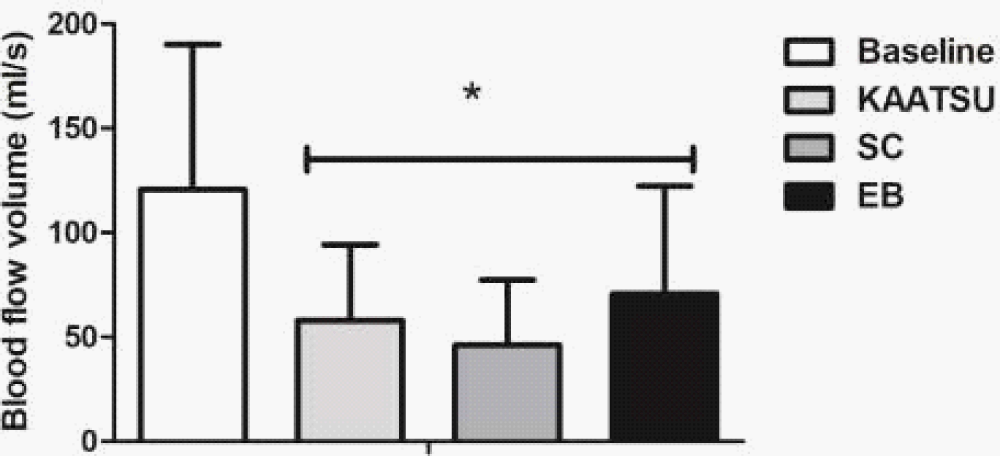
Figure 2: Blood flow volume values as the mean and SD±. KAATSU in optimal pressure; SC: sphygmomanometer cuff; EB: elastic band. * Significant difference from baseline (p < 0.05).
Diameter of the brachial artery
There was no significant change in the brachial artery diameter in the KA (2.1%, S: 0.08, CI: 0.43 – 0.48 cm; p = 0.958), SC (4.2%, ES: 0.28, CI: 0.42 – 0.46 cm, p = 0.486), or EB (2.1%, ES: 0.18, CI: 0.43 – 0.47 cm, p = 0.674) (Figure 3).
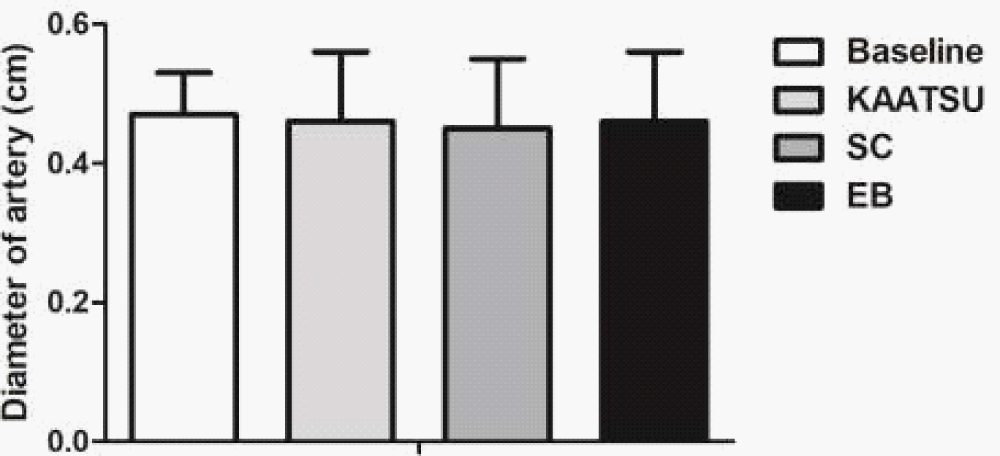
Figure 3: Diameter of brachial artery. KAATSU in optimal pressure; SC: Sphygmomanometer Cuff; EB: Elastic Band (p > 0.05).
No significant difference was observed between conditions (p > 0.05). The test-retest reliability of the diameter of the artery using SEM, MD, and CV% were 0.03 cm, 0.1 cm, and 0.5%, respectively.
Blood flow velocity
There was a significant time effect for blood flow velocity (p < 0.0001) with no interaction condition*time (p > 0.05).
Blood flow velocity was significantly reduced in the KA (52%, ES: 0.74, CI: 57.0 – 69.0 cm/s, p < .0001), SC (61.7%, ES: 1.02, CI: 53.1 – 65.1 cm/s, p < .0001), and EB (41.5%, ES: 1.02, CI: 53.4 – 65.4 cm/s p < .0001). No significant difference was observed between conditions (p = 0.460) (Figure 4). The test-retest reliability of blood flow velocity using SEM, MD, and CV% were 13.9 cm/s, 38.5 cm/s, and 0.9%, respectively.
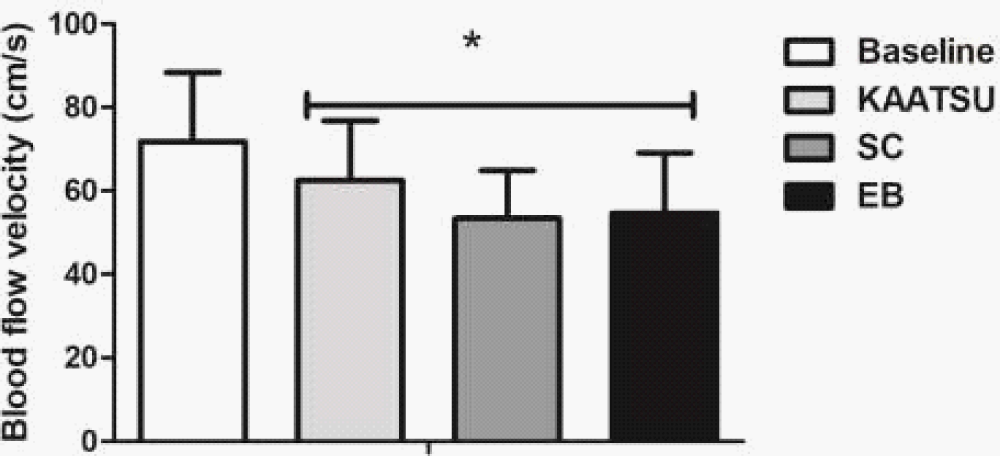
Figure 4: Blood flow velocity values as the mean and SD±. KAATSU in optimal pressure; SC: Sphygmomanometer Cuff; EB: Elastic Band. * Significant difference from baseline (p < 0.05).
The aim of this study was to investigate whether the vascular parameters regarding blood flow volume, velocity and diameter of the brachial artery during blood flow restriction using pneumatic controlled cuff-KAATSU, sphygmomanometer cuff, and an elastic band at the same perceived tightness were similar.
In the present study, we observed a reduction in blood flow and blood flow velocity, while the brachial diameter of the artery did not change by applying KA, SC, and EB cuffs at the same perceived tightness. Taken together, these results suggest that standardizing the perceived tightness and cuff width on the upper arms could result in a similar restriction stimulus regardless of cuff type. Our findings are in accordance with some studies in the literature [17,20]. For example, Abe, et al. [20] reported that the reduction in resting brachial blood flow and peak blood velocity were similar when an elastic cuff was pulled to 10%/20% of its initial length compared to a pressurized nylon cuff (CC) inflated to 40%/80% of AOP, with no significant difference between cuffs. Participants using KA, SC, and EB in KOP rated the PT at 4.2, 4.2, and 4.3, respectively, on the perceived scale, and none of the participants achieved brachial artery occlusion. These levels of perceived tightness were lower than those reported by Wilson, et al. [12] and might be related to the fact that the authors studied lower limb pressure instead of upper limb pressure. It also might be pointed out that the studied subjects had a BMI of > 26 and they were not healthy active male participants, and this may interfere with the results although, the weight would have higher interference in the lower limbs measures which was not the case.
Congruent with our findings, Bell, et al. [17], using a large sample size (58 men and 62 women), reported that when the participants rated 7 out of 10 on the PT scale proposed by Wilson, et al. [12] in the upper body, the mean percentage of arterial occlusion pressure was 92 mmHg (86.9% of AOP).
The variety of devices used in the BFR technique may present benefits, but some pneumatic cuffs, such as KA, may not be practical or accessible compared to other cuffs due to the high cost and the need for professionals’ specific expertise and training. However, there is some criticism of EB use in the BFR literature [17] because of the unknown amount of blood flow restriction induced by EB. Our results showed that EB could be a feasible alternative to conventional cuffs.
BFR has been identified as an interesting technique to induce increases in strength and muscle hypertrophy in young [8,21,22], athletes [23] and even in populations with some musculoskeletal and cardiovascular limitations [11,24,25] and other chronic degenerative diseases [7,26,27].
One of the advantages of low-load resistance training with BFR is that it allows people who are unable to lift high loads to achieve muscular adaptations in a similar way to those who use high loads [28], without negative vascular effects, since resistance exercises with high loads can lead to arterial stiffness with an increased central pulse pressure [29,30]. This is because, although BFR with low-load resistance exercise promotes hypoxemia during cuff compression and consequently increases sympathetic activity and subsequent vasoconstriction, after its decompression, nitric oxide and endothelial growth factor are released, acting as vascular protectors and promoting angiogenesis.
Regarding BFR methodology, one of the most important points is how to do the restriction per se and achieve the optimal restriction pressure for each person to acquire the expected result regarding muscle resistance or aerobic improvement, without harm to the vascular system, while the blood flow restriction is done [31,32]. It has already been shown that some variables interfere with the blood flow restriction technique. Limb position and temperature, the way that cuff application is made in the limb, and tourniquet cuff shape, width, and length are some of them [19,33]. Patterson, et al. [34] published a blood flow restriction exercise guideline focusing on the methodology, application, and safety of this mode of training on muscular strength and hypertrophy. In short, it was concluded that there is a wide variety of applied pressure, width cuffs, and other variables used in protocols, which increases the difficulty of comparing results and affects their reproducibility.
In the BFR technique, some devices are used, such as KAATSU, Delfi, and Hokanson, Vasper [2] that are electronically controlled. These devices may more precisely control the amount of pressure that is being applied to the limb. Although these devices present significant differences between measurement units for limb occlusion pressure (Delfi: 239.4 mmHg vs. KAATSU: 500 mmHg) [19], reassuring how important it is to study each of the devices, their pressures and equivalence during the restriction to make the technique more reproducible and popular. Comparison between blood flow restriction cuffs and the understanding of their similarity is important to allow the technique to be used safely and by more individuals.
In conclusion, our results showed similar brachial blood flow behavior among KA, SC, and EB at the same perceived tightness. However, longitudinal and randomized studies are needed to compare the training effects between them. Our study would facilitate the reproducibility of the BFR technique, regardless of the device used which might facilitate clinical use, with less cost (the SC is cheaper) and more accessible. All the cuffs were similar in the measures studied and safe regarding the technique.
Strengths and limitations
This study is not without limitations. First, our findings are specific to young healthy men, and it, therefore, is unclear to what extent these results can be extrapolated to other populations, such as untrained, elderly, women, or clinical settings. Second, the perceived tightness scale was originally implemented for use with an elastic band on the lower body (quadriceps) and it is important to note that there is a subjective nature of the perceived tightness technique that might had its interference in the results. One study mentioned that the participants rated changes in perceived tightness over multiple visits during elastic band use (Bell et al., 2020). The same authors supported the utility of the method as a means for the completion of practical blood flow restriction (Bell et al,2018) once it is easy to use, with less cost and it is similar to those used in literature that might need more expensive equipment and demand more training to use. However, it is worth mentioning that perceived tightness with KAATSU was measured previously as a reference to match PT in both EB and SC measurements.
This research was partially financed by the SEED Money program (for young researchers).
- Sato Y. The history and future of KAATSU Training. International Journal of KAATSU Training Research. 2005; 1(1): 1–5. https://doi.org/10.3806/ijktr.1.1
- Gladden J, Wernecke C, Rector S, Tecson K, McCullough P. Pilot safety study: The use of Vasper, a novel blood flow restriction exercise, in healthy adults. J Exerc Phys. 2016; 19(2):99–105
- McEwen JA, Owens JG, Jeyasurya J. Why is it Crucial to Use Personalized Occlusion Pressures in Blood Flow Restriction (BFR) Rehabilitation? Journal of Medical and Biological Engineering. 2018, April 9; 39(2):173–177. https://doi.org/10.1007/s40846-018-0397-7
- Wernbom M, Apro W, Paulsen G, Nilsen TS, Blomstrand E, Raastad T. Acute low-load resistance exercise with and without blood flow restriction increased protein signalling and number of satellite cells in human skeletal muscle. Eur J Appl Physiol. 2013 Dec;113(12):2953-65. doi: 10.1007/s00421-013-2733-5. PMID: 24078212.
- Jessee MB, Buckner SL, Mouser JG, Mattocks KT, Dankel SJ, Abe T, Bell ZW, Bentley JP, Loenneke JP. Muscle Adaptations to High-Load Training and Very Low-Load Training With and Without Blood Flow Restriction. Front Physiol. 2018 Oct 16;9:1448. doi: 10.3389/fphys.2018.01448. PMID: 30386254; PMCID: PMC6198179.
- Nakajima T, Kurano M, Iida H, Takano H, Oonuma H, Morita T, Meguro K, Sato Y, Nagata T, KAATSU Training Group. Use and safety of KAATSU training:Results of a national survey. International Journal of KAATSU Training Research. 2006; 2(1):5–13. https://doi.org/10.3806/ijktr.2.5
- Yow BG, Tennent DJ, Dowd TC, Loenneke JP, Owens JG. Blood Flow Restriction Training After Achilles Tendon Rupture. J Foot Ankle Surg. 2018 May-Jun;57(3):635-638. doi: 10.1053/j.jfas.2017.11.008. Epub 2018 Feb 21. PMID: 29477554.
- Takarada Y, Nakamura Y, Aruga S, Onda T, Miyazaki S, Ishii N. Rapid increase in plasma growth hormone after low-intensity resistance exercise with vascular occlusion. J Appl Physiol (1985). 2000 Jan;88(1):61-5. doi: 10.1152/jappl.2000.88.1.61. PMID: 10642363.
- Takarada Y, Takazawa H, Ishii N. Applications of vascular occlusion diminish disuse atrophy of knee extensor muscles. Med Sci Sports Exerc. 2000 Dec;32(12):2035-9. doi: 10.1097/00005768-200012000-00011. PMID: 11128848.
- Shinohara M, Kouzaki M, Yoshihisa T, Fukunaga T. Efficacy of tourniquet ischemia for strength training with low resistance. Eur J Appl Physiol Occup Physiol. 1998;77(1-2):189-91. doi: 10.1007/s004210050319. PMID: 9459541.
- Rossow LM, Fahs CA, Loenneke JP, Thiebaud RS, Sherk VD, Abe T, Bemben MG. Cardiovascular and perceptual responses to blood-flow-restricted resistance exercise with differing restrictive cuffs. Clin Physiol Funct Imaging. 2012 Sep;32(5):331-7. doi: 10.1111/j.1475-097X.2012.01131.x. Epub 2012 Apr 4. PMID: 22856338.
- Wilson JM, Lowery RP, Joy JM, Loenneke JP, Naimo MA. Practical blood flow restriction training increases acute determinants of hypertrophy without increasing indices of muscle damage. J Strength Cond Res. 2013 Nov;27(11):3068-75. doi: 10.1519/JSC.0b013e31828a1ffa. PMID: 23446173.
- Lowery RP, Joy JM, Loenneke JP, de Souza EO, Machado M, Dudeck JE, Wilson JM. Practical blood flow restriction training increases muscle hypertrophy during a periodized resistance training programme. Clin Physiol Funct Imaging. 2014 Jul;34(4):317-21. doi: 10.1111/cpf.12099. Epub 2013 Nov 4. PMID: 24188499.
- Lixandrão ME, Ugrinowitsch C, Berton R, Vechin FC, Conceição MS, Damas F, Libardi CA, Roschel H. Magnitude of Muscle Strength and Mass Adaptations Between High-Load Resistance Training Versus Low-Load Resistance Training Associated with Blood-Flow Restriction: A Systematic Review and Meta-Analysis. Sports Med. 2018 Feb;48(2):361-378. doi: 10.1007/s40279-017-0795-y. PMID: 29043659.
- Stray-Gundersen S, Wooten S, Tanaka H. Walking With Leg Blood Flow Restriction: Wide-Rigid Cuffs vs. Narrow-Elastic Bands. Front Physiol. 2020 May 29;11:568. doi: 10.3389/fphys.2020.00568. PMID: 32547424; PMCID: PMC7273976.
- Bell ZW, Dankel SJ, Mattocks KT, Buckner SL, Jessee MB, Mouser JG, Abe T, Loenneke JP. An investigation into setting the blood flow restriction pressure based on perception of tightness. Physiol Meas. 2018 Oct 19;39(10):105006. doi: 10.1088/1361-6579/aae140. PMID: 30211696.
- Bell ZW, Dankel SJ, Spitz RW, Chatakondi RN, Abe T, Loenneke JP. The Perceived Tightness Scale Does Not Provide Reliable Estimates of Blood Flow Restriction Pressure. J Sport Rehabil. 2019 Sep 24;29(4):516-518. doi: 10.1123/jsr.2018-0439. PMID: 31553951.
- Thijssen DH, Black MA, Pyke KE, Padilla J, Atkinson G, Harris RA, Parker B, Widlansky ME, Tschakovsky ME, Green DJ. Assessment of flow-mediated dilation in humans: a methodological and physiological guideline. Am J Physiol Heart Circ Physiol. 2011 Jan;300(1):H2-12. doi: 10.1152/ajpheart.00471.2010. Epub 2010 Oct 15. PMID: 20952670; PMCID: PMC3023245.
- Weatherholt AM, Vanwye WR, Lohmann J, Owens JG. The Effect of Cuff Width for Determining Limb Occlusion Pressure: A Comparison of Blood Flow Restriction Devices. Int J Exerc Sci. 2019 Jan 1;12(3):136-143. PMID: 30761200; PMCID: PMC6355123.
- Abe T, Mouser JG, Dankel SJ, Bell ZW, Buckner SL, Mattocks KT, Jessee MB, Loenneke JP. A method to standardize the blood flow restriction pressure by an elastic cuff. Scand J Med Sci Sports. 2019 Mar;29(3):329-335. doi: 10.1111/sms.13340. Epub 2018 Dec 9. PMID: 30468528.
- Laurentino GC, Loenneke JP, Teixeira EL, Nakajima E, Iared W, Tricoli V. The Effect of Cuff Width on Muscle Adaptations after Blood Flow Restriction Training. Med Sci Sports Exerc. 2016 May;48(5):920-5. doi: 10.1249/MSS.0000000000000833. PMID: 26656773.
- Conceição MS, Junior EMM, Telles GD, Libardi CA, Castro A, Andrade ALL, Brum PC, Urias Ú, Kurauti MA, Júnior JMC, Boschero AC, Cavaglieri CR, Camera DM, Chacon-Mikahil MPT. Augmented Anabolic Responses after 8-wk Cycling with Blood Flow Restriction. Med Sci Sports Exerc. 2019 Jan;51(1):84-93. doi: 10.1249/MSS.0000000000001755. PMID: 30113523.
- Scott BR, Loenneke JP, Slattery KM, Dascombe BJ. Blood flow restricted exercise for athletes: A review of available evidence. J Sci Med Sport. 2016 May;19(5):360-7. doi: 10.1016/j.jsams.2015.04.014. Epub 2015 May 9. PMID: 26118847.
- Barbalho M, Rocha AC, Seus TL, Raiol R, Del Vecchio FB, Coswig VS. Addition of blood flow restriction to passive mobilization reduces the rate of muscle wasting in elderly patients in the intensive care unit: a within-patient randomized trial. Clin Rehabil. 2019 Feb;33(2):233-240. doi: 10.1177/0269215518801440. Epub 2018 Sep 24. PMID: 30246555.
- Centner C, Wiegel P, Gollhofer A, König D. Correction to: Effects of Blood Flow Restriction Training on Muscular Strength and Hypertrophy in Older Individuals: A Systematic Review and Meta-Analysis. Sports Med. 2019 Jan;49(1):109-111. doi: 10.1007/s40279-018-1013-2. Erratum for: Sports Med. 2019 Jan;49(1):95-108. PMID: 30414044; PMCID: PMC6828275.
- Noto T, Hashimoto G, Takagi T, Awaya T, Araki T, Shiba M, Iijima R, Hara H, Moroi M, Nakamura M, Sugi K. Paget-Schroetter Syndrome Resulting from Thoracic Outlet Syndrome and KAATSU Training. Intern Med. 2017 Oct 1;56(19):2595-2601. doi: 10.2169/internalmedicine.7937-16. Epub 2017 Sep 6. PMID: 28883228; PMCID: PMC5658525.
- Fukuda T, Yasuda T, Fukumura K, Iida H, Morita T, Sato Y, Nakajima T. Low-intensity kaatsu resistance exercises using an elastic band enhance muscle activation in patients with cardiovascular diseases. International Journal of KAATSU Training Research. 2013; 9(1):1–5. https://doi.org/10.3806/ijktr.9.1
- Pereira-Neto EA, Lewthwaite H, Boyle T, Johnston K, Bennett H, Williams MT. Effects of exercise training with blood flow restriction on vascular function in adults: a systematic review and meta-analysis. PeerJ. 2021 Jul 7;9:e11554. doi: 10.7717/peerj.11554. PMID: 34277146; PMCID: PMC8272459.
- Miyachi M, Donato AJ, Yamamoto K, Takahashi K, Gates PE, Moreau KL, Tanaka H. Greater age-related reductions in central arterial compliance in resistance-trained men. Hypertension. 2003 Jan;41(1):130-5. doi: 10.1161/01.hyp.0000047649.62181.88. PMID: 12511542.
- Miyachi M, Kawano H, Sugawara J, Takahashi K, Hayashi K, Yamazaki K, Tabata I, Tanaka H. Unfavorable effects of resistance training on central arterial compliance: a randomized intervention study. Circulation. 2004 Nov 2;110(18):2858-63. doi: 10.1161/01.CIR.0000146380.08401.99. Epub 2004 Oct 18. PMID: 15492301.
- Fahs CA, Loenneke JP, Rossow LM, Tiebaud RS, Bemben MG. Methodological considerations for blood flow restricted resistance exercise. Journal of Trainology. 2012; 1(1):14–22. https://doi.org/10.17338/trainology.1.1_14
- Loenneke JP, Fahs CA, Rossow LM, Thiebaud RS, Mattocks KT, Abe T, Bemben MG. Blood flow restriction pressure recommendations: a tale of two cuffs. Front Physiol. 2013 Sep 10;4:249. doi: 10.3389/fphys.2013.00249. PMID: 24058346; PMCID: PMC3767914.
- Loenneke JP, Fahs CA, Rossow LM, Sherk VD, Thiebaud RS, Abe T, Bemben DA, Bemben MG. Effects of cuff width on arterial occlusion: implications for blood flow restricted exercise. Eur J Appl Physiol. 2012 Aug;112(8):2903-12. doi: 10.1007/s00421-011-2266-8. Epub 2011 Dec 6. PMID: 22143843; PMCID: PMC4133131.
- Patterson SD, Hughes L, Warmington S, Burr J, Scott BR, Owens J, Abe T, Nielsen JL, Libardi CA, Laurentino G, Neto GR, Brandner C, Martin-Hernandez J, Loenneke J. Blood Flow Restriction Exercise: Considerations of Methodology, Application, and Safety. Front Physiol. 2019 May 15;10:533. doi: 10.3389/fphys.2019.00533. Erratum in: Front Physiol. 2019 Oct 22;10:1332. PMID: 31156448; PMCID: PMC6530612.