
More Information
Submitted: April 25, 2023 | Approved: June 07, 2023 | Published: June 08, 2023
How to cite this article: Forkapa K, Carnahan S. Collegiate athlete with unilateral swollen arm after exercise. J Sports Med Ther. 2023; 8: 021-023.
DOI: 10.29328/journal.jsmt.1001067
Copyright License: © 2023 Forkapa K, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Thoracic outlet; McCleery; Paget-Schroetter; Extremity swelling

Collegiate athlete with unilateral swollen arm after exercise
Kristin Forkapa* and Sean Carnahan
University of Pittsburgh Medical Center, Pittsburgh, PA, USA
*Address for Correspondence: Kristin Forkapa, DO, University of Pittsburgh Medical Center, Pittsburgh, PA, USA, Email: [email protected]
A collegiate football player presented to the athletic training room with the complaint of intermittent left upper extremity swelling. Deep vein thromboses as well as abnormalities of the cervical spine were ruled out initially. He was referred to a vascular surgeon and diagnosed with McCleery Syndrome after evaluation of the thoracic outlet with dynamic ultrasound testing. He was treated surgically for decompression of his venous thoracic outlet syndrome and has since made a full recovery.
Upper extremity swelling due to thoracic outlet occlusion is an uncommon presentation in athletes. However, when it does present it is typically seen in athletes with repetitive overhead motion comprised of abduction and external rotation. This is common in weightlifting, baseball, swimming, and football [1]. Differential diagnoses of isolated upper extremity swelling can include deep vein thrombosis, thoracic outlet syndrome (including both Paget-Schroetter Syndrome and McCleery Syndrome), or neurologic compression. A thorough history and physical exam, as well as appropriate imaging and dynamic testing, are necessary to accurately identify the causes of thoracic outlet syndrome. Management of thoracic outlet syndrome varies depending on the underlying causes, but ranges from conservative therapy to surgical decompression; most cases require a multimodal approach [2].
A 19-year-old right-hand dominant male Division 1 college football athlete with no significant past medical history presents to the training room with the complaint of a swollen left arm for the past 3 days (Figures 1-3). He states that it happened without any identifiable trigger, trauma, or inciting event. However, he did several sessions of upper-body weight training earlier in the week consisting of overhead and chest presses. He denies pain, warmth, erythema, weakness, bruising, or pruritis of the skin. He does complain of intermittent numbness in his hand. He also reports no recent illness or fever, chills, or night sweats. Of note, he does report a similar experience of his left chest/shoulder after exercise in the prior year. Of note, the athlete did provide consent for this study.
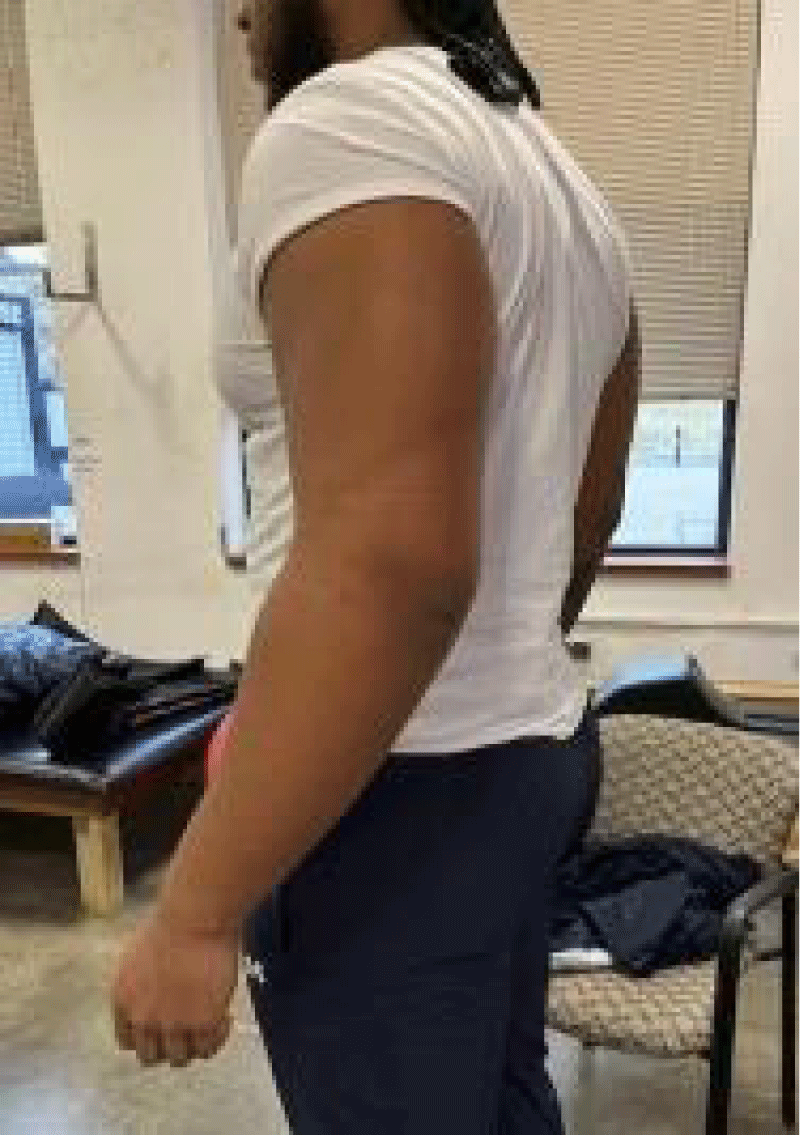
Figure 1: Lateral view of left upper extremity.
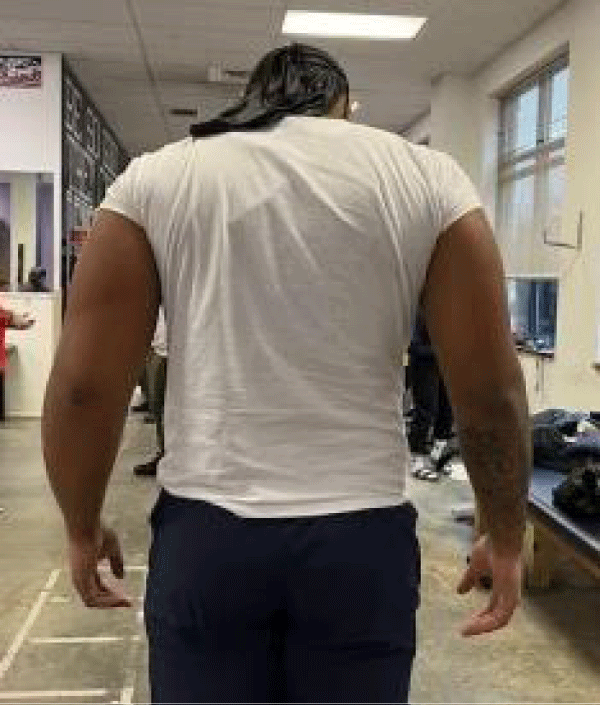
Figure 2: Posterior view of bilateral upper extremities, indicating the left swollen extremity in comparison.

Figure 3: Anterior view of bilateral upper extremities, indicating the left swollen extremity in comparison.
Physical exam, initial evaluation
In the training room at his initial presentation, his physical exam showed swelling of the left upper extremity spanning from the mid-forearm to the axilla. The was no erythema, bruising, or hematomas present. No dilated chest wall veins. Capillary refill was brisk and +2 radial pulse was present. Full range of motion with +5/5 strength in forward flexion, abduction, and internal and external rotation was present. No sensory deficits were noted. After evaluation in the training room, the initial study ordered a radiograph of the left shoulder and cervical spine, both of which had no abnormalities. An ultrasound venous duplex scan of the left upper extremity was also ordered, which was negative for thrombosis. He presented to the Emergency Department later that evening for worsening symptoms, and a CT scan of the chest with contrast was performed, which was also negative. After a review of his negative studies by the team physician the next day, he was referred to a vascular surgeon for further evaluation of potential thoracic outlet syndrome.
He had a dynamic venous duplex ultrasound performed in the clinic with the specialist, which did have notable findings. Again there was no deep vein thrombosis seen while laying supine, however, when the athlete was sitting, elevated velocities were seen in the proximal axillary vein with compression of the vein seen with collaterals. With the arm abducted to 90 degrees, there was continuous but slowed flow within the axillary vein, concerning McCleery Syndrome. He was later on scheduled for a same-day venogram, followed by surgical intervention for left venous thoracic outlet syndrome decompression. This included left first rib resection, subclavius muscle resection, and venolysis of the left subclavian vein. His postoperative course was uncomplicated, and he has since made a full recovery.
Thoracic outlet syndrome refers to different types of compressive pathology occurring at the thoracic outlet. It can be further subdivided into venous, arterial, or neurogenic thoracic outlet syndrome. Venous thoracic outlet syndrome can also be further subdivided into Paget-Schroetter Syndrome and McCleery Syndrome. Overall, neurogenic thoracic outlet syndrome is the most common, accounting for about 90% of all thoracic outlet cases [3]. McCleery Syndrome is caused by compression of the subclavian vein between the clavicle and the first rib at the costoclavicular space. This can be due to different anatomical variables, including an abnormal insertion of the costoclavicular ligament or muscular hypertrophy of the anterior scalene or subclavius. Symptoms are intermittent, based on activity and degree of venous compression. However, while McCleery Syndrome is diagnosed by a lack of thrombosis, there is a concern for the development of such complications due to the nature of frequent obstruction and hemostasis [4]. Thus, it is recommended that patients are treated surgically with first rib resection and/or scalenectomy [5]. Paget-Schroetter Syndrome is another subtype of venous thoracic outlet syndrome; however, it is differentiated from McCleery Syndrome by the presence of a thrombus. Repetitive vigorous physical activity that causes frequent compression of the subclavian vein can cause venous injury and thus thrombosis. The differentiation of McCleery Syndrome vs. Paget-Schroetter Syndrome is done by venous ultrasonography [6]. Overall, the rates of venous thoracic outlet syndrome in past years have been approximately 8 per year in a metropolitan demographic of 1,000,000 [7]. Other possible diagnoses to be considered with this presentation of upper extremity swelling include brachial plexopathy. Brachial plexopathy refers to a dysfunction of the brachial plexus. It can be attributed to several mechanisms- including direct trauma, compression by surrounding anatomical structures (commonly the scalene triangle, between the clavicle and first rib, or the infraclavicular pectoralis minor space [8]), as well as idiopathic causes. Patients typically have neurological symptoms within the C5-T1 nerve roots, including paresthesia or pain [9]. Brachial plexopathy due to compression of the thoracic outlet in the setting of the repetitive motion of the upper extremity is termed neurogenic thoracic outlet syndrome [10]. Compression is typically due to obstruction by the clavicle, first rib, and scalene muscles [11]. While evaluation of venous thoracic outlet syndrome is completed with duplex imaging (as a replacement for invasive angiographic approaches), and neurogenic thoracic outlet syndrome is completed by electrophysiological nerve studies [12]. As with this patient who was diagnosed with McCleery syndrome, definitive management occurs with surgical intervention, however, there are other conservative options. Non-surgical treatment options can include physical therapy, weight loss, anti-inflammatory medications, and botulinum toxin injections [13]. Regarding surgical management, studies have shown excellent symptom resolution after surgical management, with about 83.3% reporting no symptoms at six months [14]. Regarding an athlete’s return to sport, the average return time is about 12 weeks post-operatively with appropriate and consistent physical therapy [15].
After imaging and dynamic testing of the thoracic outlet, the athlete was diagnosed with McCleery syndrome. He underwent definitive surgical management via resection of his first rib and subclavius muscle, as well as venolysis of the subclavian vein. He has since made an excellent recovery and continues to participate in sporting activities and exercise without complication.
We would like to acknowledge the athletic training staff at Robert Morris University.
- Keller RE, Croswell DP, Medina GIS, Cheng TTW, Oh LS. Paget-Schroetter syndrome in athletes: a comprehensive and systematic review. J Shoulder Elbow Surg. 2020 Nov;29(11):2417-2425. doi: 10.1016/j.jse.2020.05.015. Epub 2020 Jun 9. PMID: 32868012.
- Jones MR, Prabhakar A, Viswanath O, Urits I, Green JB, Kendrick JB, Brunk AJ, Eng MR, Orhurhu V, Cornett EM, Kaye AD. Thoracic Outlet Syndrome: A Comprehensive Review of Pathophysiology, Diagnosis, and Treatment. Pain Ther. 2019 Jun;8(1):5-18. doi: 10.1007/s40122-019-0124-2. Epub 2019 Apr 29. PMID: 31037504; PMCID: PMC6514035.
- Kaplan J, Kanwal A. Thoracic Outlet Syndrome. [Updated 2023 Apr 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. https://www.ncbi.nlm.nih.gov/books/NBK557450/
- Allam AK, Ismail MIM, Abd El-Salam Rizk MAM. McCleery‘s Syndrome the Overlooked Cause of Swollen Upper Limb, Completion Venoplasty is The Key Word for Successful Surgical Decompression. The Egyptian Journal of Hospital Medicine. 2021 October. 85 (2): 3790-3797.
- Likes K, Rochlin DH, Call D, Freischlag JA. McCleery syndrome: etiology and outcome. Vasc Endovascular Surg. 2014 Feb;48(2):106-10. doi: 10.1177/1538574413512380. Epub 2013 Dec 12. PMID: 24334914.
- Saleem T, Baril DT. Paget Schroetter Syndrome. [Updated 2022 Jan 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan- https://www.ncbi.nlm.nih.gov/books/NBK482416/
- Illig KA, Rodriguez-Zoppi E, Bland T, Muftah M, Jospitre E. The Incidence of Thoracic Outlet Syndrome. Ann Vasc Surg. 2021 Jan;70:263-272. doi: 10.1016/j.avsg.2020.07.029. Epub 2020 Aug 6. PMID: 32771464.
- Ohman JW, Thompson RW. Thoracic Outlet Syndrome in the Overhead Athlete: Diagnosis and Treatment Recommendations. Curr Rev Musculoskelet Med. 2020 Aug;13(4):457-471. doi: 10.1007/s12178-020-09643-x. PMID: 32514995; PMCID: PMC7340704.
- Khadilkar SV, Khade SS. Brachial plexopathy. Ann Indian Acad Neurol. 2013 Jan;16(1):12-8. doi: 10.4103/0972-2327.107675. PMID: 23661957; PMCID: PMC3644772.
- Shutze W, Richardson B, Shutze R, Tran K, Dao A, Ogola GO, Young A, Pearl G. Midterm and long-term follow-up in competitive athletes undergoing thoracic outlet decompression for neurogenic thoracic outlet syndrome. J Vasc Surg. 2017 Dec;66(6):1798-1805. doi: 10.1016/j.jvs.2017.06.108. Epub 2017 Sep 21. PMID: 28943009.
- Garraud T, Pomares G, Daley P, Menu P, Dauty M, Fouasson-Chailloux A. Thoracic Outlet Syndrome in Sport: A Systematic Review. Front Physiol. 2022 Jun 8;13:838014. doi: 10.3389/fphys.2022.838014. PMID: 35755427; PMCID: PMC9214221.
- Klaassen Z, Sorenson E, Tubbs RS, Arya R, Meloy P, Shah R, Shirk S, Loukas M. Thoracic outlet syndrome: a neurological and vascular disorder. Clin Anat. 2014 Jul;27(5):724-32. doi: 10.1002/ca.22271. Epub 2013 May 29. PMID: 23716186.
- Panther EJ, Reintgen CD, Cueto RJ, Hao KA, Chim H, King JJ. Thoracic outlet syndrome: a review. J Shoulder Elbow Surg. 2022 Nov;31(11):e545-e561. doi: 10.1016/j.jse.2022.06.026. Epub 2022 Aug 10. PMID: 35963513.
- Talutis SD, Ulloa JG, Gelabert HA. Adolescent athletes can get back in the game after surgery for thoracic outlet syndrome. J Vasc Surg. 2023 Feb;77(2):599-605. doi: 10.1016/j.jvs.2022.10.002. Epub 2022 Oct 12. PMID: 36243264.
- Hock G, Johnson A, Barber P, Papa C. Current Clinical Concepts: Rehabilitation of Thoracic Outlet Syndrome. J Athl Train. 2022 Nov 17. doi: 10.4085/1062-6050-138-22. Epub ahead of print. PMID: 36395374.