
More Information
Submitted: April 05, 2023 | Approved: April 20, 2023 | Published: April 21, 2023
How to cite this article: Xu X, Xu J. Effects of exercise on wall shear stress in male and female patients with coronary heart disease. J Sports Med Ther. 2023; 8: 004-007.
DOI: 10.29328/journal.jsmt.1001064
Copyright License: © 2023 Xu X, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Exercise; Sex; Coronary heart disease; Wall shear stress; Endothelial

Effects of exercise on wall shear stress in male and female patients with coronary heart disease
Xiuxiu Xu1 and Jiaquan Xu2*
1Department of Rehabilitation Medicine, The First Affiliated Hospital of Nanchang University, Nanchang 330006, People’s Republic of China
2Jiangxi Key Laboratory for Mass Spectrometry and Instrumentation, East China University of Technology, Nanchang 330013, People’s Republic of China
*Address for Correspondence: Jiaquan Xu, Jiangxi Key Laboratory for Mass Spectrometry and Instrumentation, East China University of Technology, Nanchang 330013, People’s Republic of China, Email: [email protected]
Coronary heart disease (CHD) seriously endangers human health, and there are obvious gender differences in incidence rate and prognosis, which are related to the evident differences in anatomical structure, physiological characteristics, and wall shear stress between males and females. In recent years, cardiac rehabilitation has been proven to be safe and effective in controlling the progression and improving the prognosis of CHD. Thereinto, exercise therapy is the central link of cardiac rehabilitation. Exercise can significantly affect vascular endothelial function by regulating wall shear stress. Based on previous research, this paper will briefly review the influence of exercise on wall shear stress in male and female patients with CHD, in order to provide a reference for formulating personalized cardiac rehabilitation programs and further improve the prognosis of CHD.
Coronary Heart Disease (CHD) is a cardiovascular disease with the highest mortality in the world, which has significant gender differences in the incidence rate and prognosis [1]. According to research data, female patients with CHD have a higher probability of developing myocardial infarction or fatal CHD than males with age [1]. It has been confirmed that coronary endothelial dysfunction is the key to the occurrence of atherosclerotic plaque. Repeated exposure of endothelial cells to blood flow stimuli leads to adaptive changes in vascular function and structure. The flow of blood in the lumen generates mechanical stimuli that act in various directions of the vessel wall, mainly including Wall Shear Stress (WSS) parallel to the blood flow direction and cross-wall pressure perpendicular to the vessel wall (Figure 1) [2]. Researches indicate that WSS plays an important role in the regulation of vascular endothelial function, promoting or inhibiting the formation of coronary atherosclerotic plaque [3,4]. In addition, some researchers believe that exercise can induce sharp changes in WSS, trigger endothelial receptors, and thus affect the function of endothelial cells [5]. A large number of sports physiological studies have confirmed that long-term regular and reasonable exercise can reduce arterial stiffness, increase vascular elasticity, and thereby decrease the risk of cardiovascular disease [6-8]. Therefore, this paper briefly summarizes the effects of exercise intensities on WSS in male and female patients with CHD, to provide a theoretical basis for establishing personalized cardiac rehabilitation programs for patients with CHD in the future.
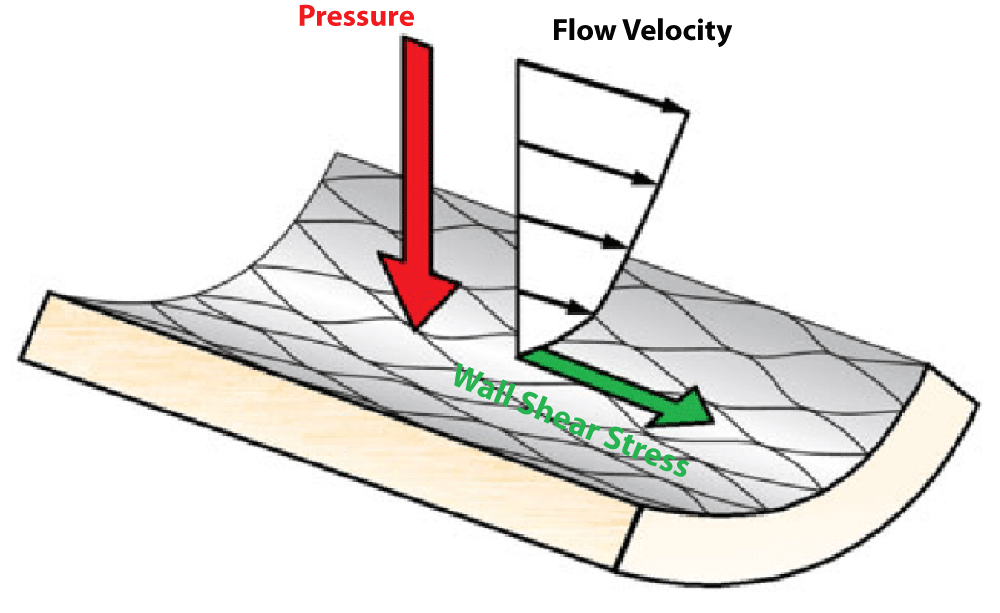
Figure 1: Diagram of forces on the wall of a blood vessel [2].
Effects of exercise on WSS in patients with CHD
Exercise is an important means of non-invasive cardiovascular disease prevention, which can cause changes in WSS, and this change is related to exercise intensity. Endothelial located in the innermost layer of the vascular wall can recognize different WSS signals and transmit this mechanical force signal to the interior of the cell, resulting in changes in the secretion of vasoactive substances such as nitric oxide and reactive oxygen species [9,10], which are closely related to vascular endothelial function and vascular homeostasis. Many in vivo studies have shown that WSS plays a key role in the regulation of endothelial function by exercise, and the regulation of shear force signals induced by different intensities of exercise on endothelial function and the mechanobiological mechanisms are different [11,12]. Studies have shown that the increase in exercise intensity can increase the WSS value acting on the arterial wall, resulting in changes in endothelial cell function and phenotypic adaptation [11]; On the other hand, exercise can change the direction, frequency, pulse amplitude, or blood flow pattern of blood flow to affect WSS [13]. For example, during the initial stage of the exercise, the blood flow in the vessels represents an oscillatory pattern [14], while as the exercise continues, the arterial blood flow changes to an antegrade WSS mode, which is beneficial for changes in endothelial [15]. Experiments have confirmed that endothelial cell exposed to unidirectional laminar flow WSS with a size of more than 10 dyn/cm2 shows the phenotype of anti-atherosclerosis and vascular protection, and leakage in disturbed oscillatory flow or unidirectional laminar flow WSS with the size of less than 4 dyn/cm2 is easy to activate the atherosclerotic phenotype [16-18]. Therefore, regulating endothelial function through mediating changes in WSS may be a key factor in improving cardiovascular function through exercise.
Differences in WSS between sexes
CHD is myocardial ischemia and hypoxia caused by stenosis or even occlusion of coronary artery atherosclerosis. Compared with male, female with CHD has a special pathogenesis. Emphasizing the role of gender differences in the pathogenesis of CHD is important for improving the prognosis of CHD in females. Endothelial dysfunction and hemodynamic abnormalities are common features and key events in the occurrence and development of CHD [19]. WSS, as one of the important hemodynamic parameters, is closely related to sex. Currently, many studies have proven that there are sex differences in the changes of WSS from multiple aspects. For example, Xixi Zhao, et al. conducted a cross-sectional study to monitor the mean WSS (MWSS) of the cerebral artery of 301 healthy males and females with aged between 18 and 84 years [20]. They found that MWSS in both males and females decreased significantly with age, and the most significant decrease occurred between the age range of 48-57 and 58-67. Furthermore, compared to males, females had significantly higher MWSS. Studies have shown that differences in WSS between sexes are closely related to anatomical structure, and physiological characteristics differences in the cardiovascular system. The anatomical results show that females have a smaller heart volume, coronary artery diameter, and lumen area than males [21]. The literature review written by Cheng, et al. elucidates that the value of WSS is inversely proportional to the vascular diameter (Figure 2) [22]. In addition, a 12-year longitudinal study found that the peak of WSS and MWSS decreased more significantly with age in males than in females, which was related to a more significant increase in arterial intimal thickness and degree of arteriosclerosis in females [23]. In terms of physiological function, an animal experimental study conducted by Huang A, et al. showed that estrogen in females regulates vascular dilation by stimulating the release of NO from endothelial cells, which can further affect the value of WSS [24]. These studies directly or indirectly indicate a close relationship between the mechanism of sex differences in CHD and WSS.
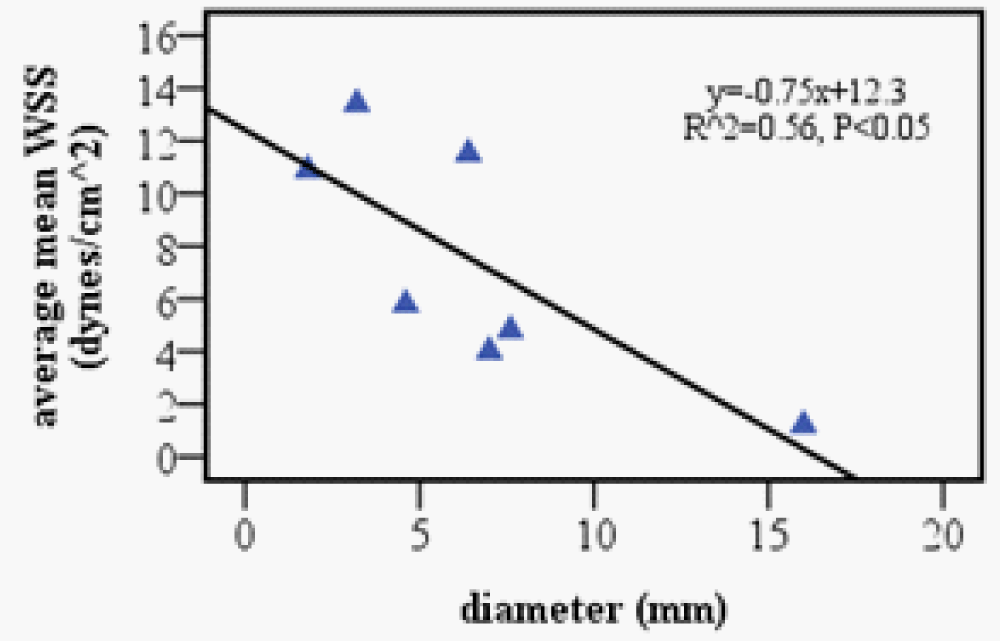
Figure 2: Relation between mean WSS and vessel lumen diameter in different types of arteries of non-atherosclerotic humans [22].
Atherosclerosis is an independent risk factor for the occurrence and development of CHD, and hemodynamic factors may be the vital factors of atherosclerosis changes, which play a key role in the formation and development of lesions. Therefore, studying the effects of exercise training on WSS is of great significance for early diagnosis and cardiac rehabilitation. Intensities of exercise have great effects on WSS. The maximum and mean values of WSS and the oscillatory WSS increase with increasing exercise intensity [25]. Research shows that moderate-intensity exercise is the most commonly recommended exercise prescription [26], which can not only reduce the damage to blood vessels caused by high-intensity exercise but also obtain higher exercise benefits. It is mainly manifested by the greater amplitude of changes in the oscillatory WSS index after high-intensity exercise, and the longer recovery time required after exercise. As mentioned earlier, there are significant differences in WSS between males and females [27], and this difference is directly or indirectly related to differences in cardiovascular between males and females [28]. Even in multivariate models that consider body surface area and control for other factors, the diameter of blood vessels in females is relatively small [21], and the vascular diameter is inversely correlated with the value of WSS [22]. However, in addition to physiological differences between sexes, differences in their lifestyle habits are also factors that cannot be ignored. Studies have shown that females are less physical activity than males [29], while exercise is an important means of preventing and improving cardiovascular disease. A randomized controlled experiment has shown that low-intensity continuous exercise can improve endothelial function in postmenopausal females, but high-intensity intermittent exercise has a better effect than moderate-intensity continuous exercise [29]. Another study based on a young obese male showed that high-intensity intermittent exercise can also significantly improve WSS and endothelial function [11]. This review mainly elaborates on the role of WSS in the process of exercise-mediated improvement of vascular endothelial function, providing a reference theoretical basis for further research on WSS with different exercise intensities. It is expected that in the future, suitable exercise prescriptions can be developed for patients with CHD, especially for female patients with specificity. At the same time, it also provides an important exercise pathway for simulating the increase of WSS in exercise scenarios.
In summary, abnormal changes in WSS are an important factor leading to endothelial cell damage in coronary arteries, and there are clear sex differences. As an important means of non-invasive prevention and treatment of cardiovascular diseases, exercise can effectively regulate changes in WSS, and this change is related to exercise intensity. Therefore, it is an important measure to improve the cardiac rehabilitation effect for male and female CHD patients by monitoring WSS and formulating personalized exercise prescriptions for cardiac rehabilitation.
I hereby declare that this piece of work was partially or fully funded by Sub-project of Key Project at Central Government Level: the ability establishment of sustainable use for valuable Chinese medicine resources with grant number: 2060302-2101-01.
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, Djousse L, Elkind MSV, Ferguson JF, Fornage M, Khan SS, Kissela BM, Knutson KL, Kwan TW, Lackland DT, Lewis TT, Lichtman JH, Longenecker CT, Loop MS, Lutsey PL, Martin SS, Matsushita K, Moran AE, Mussolino ME, Perak AM, Rosamond WD, Roth GA, Sampson UKA, Satou GM, Schroeder EB, Shah SH, Shay CM, Spartano NL, Stokes A, Tirschwell DL, VanWagner LB, Tsao CW; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020 Mar 3;141(9):e139-e596. doi: 10.1161/CIR.0000000000000757. Epub 2020 Jan 29. PMID: 31992061.
- Wang YX, Liu HB, Li PS, Yuan WX, Liu B, Liu ST, Qin KR. ROS and NO Dynamics in Endothelial Cells Exposed to Exercise-Induced Wall Shear Stress. Cell Mol Bioeng. 2018 Oct 8;12(1):107-120. doi: 10.1007/s12195-018-00557-w. PMID: 31719902; PMCID: PMC6816775.
- Shaya GE, Leucker TM, Jones SR, Martin SS, Toth PP. Coronary heart disease risk: Low-density lipoprotein and beyond. Trends Cardiovasc Med. 2022 May;32(4):181-194. doi: 10.1016/j.tcm.2021.04.002. Epub 2021 Apr 17. PMID: 33872757.
- Bertani F, Di Francesco D, Corrado MD, Talmon M, Fresu LG, Boccafoschi F. Paracrine Shear-Stress-Dependent Signaling from Endothelial Cells Affects Downstream Endothelial Function and Inflammation. Int J Mol Sci. 2021 Dec 10;22(24):13300. doi: 10.3390/ijms222413300. PMID: 34948110; PMCID: PMC8709076.
- Babbitt DM, Kim JS, Forrester SJ, Brown MD, Park JY. Effect of Interleukin-10 and Laminar Shear Stress on Endothelial Nitric Oxide Synthase and Nitric Oxide in African American Human Umbilical Vein Endothelial Cells. Ethn Dis. 2015 Nov 5;25(4):413-8. doi: 10.18865/ed.25.4.413. PMID: 26674844; PMCID: PMC4671427.
- Akyuz A. Exercise and Coronary Heart Disease. Adv Exp Med Biol. 2020;1228:169-179. doi: 10.1007/978-981-15-1792-1_11. PMID: 32342457.
- Morra EA, Zaniqueli D, Rodrigues SL, El-Aouar LM, Lunz W, Mill JG, Carletti L. Long-term intense resistance training in men is associated with preserved cardiac structure/function, decreased aortic stiffness, and lower central augmentation pressure. J Hypertens. 2014 Feb;32(2):286-93. doi: 10.1097/HJH.0000000000000035. PMID: 24351804.
- Laursen ASD, Hansen AS, Wiinberg N, Brage S, Sandbæk A, Lauritzen T, Witte DR, Jørgensen ME, Johansen NB. Higher physical activity is associated with lower aortic stiffness but not with central blood pressure: the ADDITION-Pro Study. Medicine (Baltimore). 2015 Feb;94(5):e485. doi: 10.1097/MD.0000000000000485. PMID: 25654392; PMCID: PMC4602712.
- Zhou J, Li YS, Chien S. Shear stress-initiated signaling and its regulation of endothelial function. Arterioscler Thromb Vasc Biol. 2014 Oct;34(10):2191-8. doi: 10.1161/ATVBAHA.114.303422. Epub 2014 May 29. PMID: 24876354; PMCID: PMC4169328.
- Shi W, Liu H, Cao L, He Y, Su P, Chen J, Wang M, Li X, Bai S, Tang D. Acute effect of high-intensity interval exercise on vascular endothelial function and possible mechanisms of wall shear stress in young obese males. Front Physiol. 2022 Sep 16;13:966561. doi: 10.3389/fphys.2022.966561. PMID: 36187796; PMCID: PMC9523906.
- Sakellariou XM, Papafaklis MI, Domouzoglou EM, Katsouras CS, Michalis LK, Naka KK. Exercise-mediated adaptations in vascular function and structure: Beneficial effects in coronary artery disease. World J Cardiol. 2021 Sep 26;13(9):399-415. doi: 10.4330/wjc.v13.i9.399. PMID: 34621486; PMCID: PMC8462042.
- Tang BT, Cheng CP, Draney MT, Wilson NM, Tsao PS, Herfkens RJ, Taylor CA. Abdominal aortic hemodynamics in young healthy adults at rest and during lower limb exercise: quantification using image-based computer modeling. Am J Physiol Heart Circ Physiol. 2006 Aug;291(2):H668-76. doi: 10.1152/ajpheart.01301.2005. Epub 2006 Apr 7. PMID: 16603687.
- Thijssen DH, Dawson EA, Black MA, Hopman MT, Cable NT, Green DJ. Brachial artery blood flow responses to different modalities of lower limb exercise. Med Sci Sports Exerc. 2009 May;41(5):1072-9. doi: 10.1249/MSS.0b013e3181923957. PMID: 19346980.
- Simmons GH, Padilla J, Young CN, Wong BJ, Lang JA, Davis MJ, Laughlin MH, Fadel PJ. Increased brachial artery retrograde shear rate at exercise onset is abolished during prolonged cycling: role of thermoregulatory vasodilation. J Appl Physiol (1985). 2011 Feb;110(2):389-97. doi: 10.1152/japplphysiol.00936.2010. Epub 2010 Nov 18. PMID: 21088203; PMCID: PMC3043792.
- Kumar A, Hung OY, Piccinelli M, Eshtehardi P, Corban MT, Sternheim D, Yang B, Lefieux A, Molony DS, Thompson EW, Zeng W, Bouchi Y, Gupta S, Hosseini H, Raad M, Ko YA, Liu C, McDaniel MC, Gogas BD, Douglas JS, Quyyumi AA, Giddens DP, Veneziani A, Samady H. Low Coronary Wall Shear Stress Is Associated With Severe Endothelial Dysfunction in Patients With Nonobstructive Coronary Artery Disease. JACC Cardiovasc Interv. 2018 Oct 22;11(20):2072-2080. doi: 10.1016/j.jcin.2018.07.004. Epub 2018 Sep 26. PMID: 30268874; PMCID: PMC6217963.
- Vozzi F, Campolo J, Cozzi L, Politano G, Di Carlo S, Rial M, Domenici C, Parodi O. Computing of Low Shear Stress-Driven Endothelial Gene Network Involved in Early Stages of Atherosclerotic Process. Biomed Res Int. 2018 Sep 25;2018:5359830. doi: 10.1155/2018/5359830. PMID: 30356351; PMCID: PMC6176299.
- Sahni J, Arshad M, Schake MA, Brooks JR, Yang R, Weinberg PD, Pedrigi RM. Characterizing nuclear morphology and expression of eNOS in vascular endothelial cells subjected to a continuous range of wall shear stress magnitudes and directionality. J Mech Behav Biomed Mater. 2023 Jan;137:105545. doi: 10.1016/j.jmbbm.2022.105545. Epub 2022 Oct 29. PMID: 36368188.
- Genkel VV, Kuznetcova AS, Shaposhnik II. Biomechanical Forces and Atherosclerosis: From Mechanism to Diagnosis and Treatment. Curr Cardiol Rev. 2020;16(3):187-197. doi: 10.2174/1573403X15666190730095153. PMID: 31362692; PMCID: PMC7536809.
- Zhao X, Zhao M, Amin-Hanjani S, Du X, Ruland S, Charbel FT. Wall shear stress in major cerebral arteries as a function of age and gender--a study of 301 healthy volunteers. J Neuroimaging. 2015 May-Jun;25(3):403-7. doi: 10.1111/jon.12133. Epub 2014 Jul 4. PMID: 25039410.
- Sheifer SE, Canos MR, Weinfurt KP, Arora UK, Mendelsohn FO, Gersh BJ, Weissman NJ. Sex differences in coronary artery size assessed by intravascular ultrasound. Am Heart J. 2000 Apr;139(4):649-53. doi: 10.1016/s0002-8703(00)90043-7. PMID: 10740147.
- Cheng C, Helderman F, Tempel D, Segers D, Hierck B, Poelmann R, van Tol A, Duncker DJ, Robbers-Visser D, Ursem NT, van Haperen R, Wentzel JJ, Gijsen F, van der Steen AF, de Crom R, Krams R. Large variations in absolute wall shear stress levels within one species and between species. Atherosclerosis. 2007 Dec;195(2):225-35. doi: 10.1016/j.atherosclerosis.2006.11.019. Epub 2006 Dec 12. PMID: 17169362.
- Huang A, Sun D, Koller A, Kaley G. Gender difference in flow-induced dilation and regulation of shear stress: role of estrogen and nitric oxide. Am J Physiol. 1998 Nov;275(5):R1571-7. doi: 10.1152/ajpregu.1998.275.5.R1571. PMID: 9791075.
- Irace C, Carallo C, De Franceschi MS, Scicchitano F, Milano M, Tripolino C, Scavelli F, Gnasso A. Human common carotid wall shear stress as a function of age and gender: a 12-year follow-up study. Age (Dordr). 2012 Dec;34(6):1553-62. doi: 10.1007/s11357-011-9318-1. Epub 2011 Oct 12. PMID: 21989971; PMCID: PMC3528365.
- Huang A, Sun D, Koller A, Kaley G. Gender difference in flow-induced dilation and regulation of shear stress: role of estrogen and nitric oxide. Am J Physiol. 1998 Nov;275(5):R1571-7. doi: 10.1152/ajpregu.1998.275.5.R1571. PMID: 9791075.
- Yuan W, Liu H, Luan Z, Zhao Z, Shen B. Acute Effect of High-Intensity Interval Cycling on Carotid Arterial Stiffness and Hemodynamics. Biomed Res Int. 2019 Nov 20;2019:6260286. doi: 10.1155/2019/6260286. PMID: 31998773; PMCID: PMC6970504.
- Zhou J, Li YS, Chien S. Shear stress-initiated signaling and its regulation of endothelial function. Arterioscler Thromb Vasc Biol. 2014 Oct;34(10):2191-8. doi: 10.1161/ATVBAHA.114.303422. Epub 2014 May 29. PMID: 24876354; PMCID: PMC4169328.
- Reynolds HR, Bairey Merz CN, Berry C, Samuel R, Saw J, Smilowitz NR, de Souza ACDAH, Sykes R, Taqueti VR, Wei J. Coronary Arterial Function and Disease in Women With No Obstructive Coronary Arteries. Circ Res. 2022 Feb 18;130(4):529-551. doi: 10.1161/CIRCRESAHA.121.319892. Epub 2022 Feb 17. PMID: 35175840; PMCID: PMC8911308.
- Garcia M, Mulvagh SL, Merz CN, Buring JE, Manson JE. Cardiovascular Disease in Women: Clinical Perspectives. Circ Res. 2016 Apr 15;118(8):1273-93. doi: 10.1161/CIRCRESAHA.116.307547. PMID: 27081110; PMCID: PMC4834856.
- He H, Wang C, Chen X, Sun X, Wang Y, Yang J, Wang F. The effects of HIIT compared to MICT on endothelial function and hemodynamics in postmenopausal females. J Sci Med Sport. 2022 May;25(5):364-371. doi: 10.1016/j.jsams.2022.01.007. Epub 2022 Feb 1. PMID: 35210180.