
More Information
Submitted: 17 April 2020 | Approved: 01 May 2020 | Published: 04 May 2020
How to cite this article: Magersky S. ‘Rotational alignment on patients’ clinical outcome of total knee arthroplasty: Distal femur axillary X-ray view to qualify rotation of the femoral component. J Sports Med Ther. 2020; 5: 008-011.
DOI: 10.29328/journal.jsmt.1001050
Copyright License: © 2020 Magersky S. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Arthroplasty; Malrotation; Total knee replacement

‘Rotational alignment on patients’ clinical outcome of total knee arthroplasty: Distal femur axillary X-ray view to qualify rotation of the femoral component
S Magersky*
Department of Orthopaedics, 1st Faculty of Medicine, Charles University and Na Bulovce Hospital, Czech Republic
*Address for Correspondence: S Magersky. Department of Orthopaedics, 1st Faculty of Medicine, Charles University and Na Bulovce Hospital, Budínova 2, Praha 8, 180 81, Czech Republic, Email: [email protected]
Background: Rotation of the femoral component in total knee replacement (TKR) is very important for good long-term results. Malrotation of the femoral component usually requires subsequent reimplantation. We performed X-ray projections of the knee at 90° to determine proper rotation of the femoral component without use of computed tomography.
Methods: The axial projection of the distal femur was measured in post-TKR cases. During the TKR operation, Whiteside’s method had been used to provide symmetrical flexion space. The exact outer rotation of the femoral component was measured by x-ray determination of the middle condylar twist angle, from the central epicondylar axis and posterior condylar axis.
Results: The middle condylar twist angle was in outer rotation, with an average of 3.36° (range: 1-7.6), similar to the literature. Six of the patients underwent bilateral TKR. In total, the case series included 18 women and 15 men, with average age of 71.34 years-old (range: 56-85). As a clinical evaluation we used Knee Society Score (2011). From results 2 patients were not very satisfied with the instability TKR. Axially X-ray seemed to be only which could distribute these patients.
Summary: X-ray values have the same evaluation as computed tomography. The results were 2 patients in pattern of 48, which were sufficient to extrapolate to whole population according to the statistical methods. This corresponds to 4% which we can add to evaluate satisfaction of all patients after TKR and eventually lower the total of unsatisfactory patients which is total of ¼ of total. It is also forensic reason for all patients. Our recommendation to have good results and patient satisfaction in TKR is to do x-rays before and after operation. Important are x-rays antero-posterior, lateral, and Kanekasu projection to know the rotation after TKR. Other cases without stability in flexion are nor very rarely planed for revision surgery, which is much more expensive, and burdens overall health system.
Good long-term results of total knee replacement (TKR) are reliant upon accurate positioning of the femoral component for both flexion and extension movements. For osteoarthritis cases, the TKA reduces pain for up to 15 years in 90% of the patients [1]. The remaining patients report incomplete satisfaction with their post-TKR clinical outcome [2,3], and revision rates among these patients exceed 35% within 2 years of the primary TKR [4,5]. The reported cases of loosening are mostly related to aseptic, polyethylene wear, infection, periprosthetic fracture, and joints instability.
Rotation of the femoral component in the transverse plane is a primary factor affecting post-TKR flexion stability and alignment in flexion [6-8]. Bone resection is necessary for component stability, and needs to be performed perpendicular to the preoperative biomechanical stability of the limb. Gap-balancing and measured resection are the two most commonly used methods for determination of the femoral rotation. The goal of kinematically-aligned TKR is to restore the native alignment of the limb, the knee, and the joint lines, in order to restore knee function to its native state and without ligament release. The femoral component, itself, achieves kinematic alignment when the thickness of the distal and posterior resections of the femoral condyles are equal to the thicknesses of the corresponding portions of the femoral component [9,10].
The center of knee rotation is often considered the surgical epicondylar axis (commonly referred to as the SEA), which is in effect the line connecting the sulcus of the medial epicondyle with the prominence of the lateral epicondyle [15]. The femoral component is usually implanted parallel to this line, based on anatomical landmarks [11]. For accurate determination of the SEA and proper alignment of the femoral component, the surface-delivered bony landmarks as well as the posterior condyle line and the anteroposterior trochlea axis (i.e. the Whiteside’s line) must be utilized [12]. Unfortunately, sulcus of the medial epicondyle is sometimes difficult to recognize intraoperatively and via computed tomography (CT) scan. More than 25% of reported cases of osteoarthritis of the knees were classified as type 3; meaning that the medial sulcus is not recognizable on CT scans [13]. In some cases, however, the bony landmarks technique alone can be imprecise for determining the femoral rotation alignment.
All patients involved in this study provided informed consent for participation. In total, we enrolled 50 patients, representing 48 TKR and 2 nonresponders. Six of the patients received bilateral TKR. The period of assessment was 12 months from 2017 through 2018. The sex distribution was 1.2:1, with 18 men and 15 women. The average age was 71.34 years-old (range: 56 – 85 years). All TKR were carried out in our clinic; the clinic population is representative of the population of the geographical region, increasing the likelihood that our results are transferable to the region’s whole population. The TKR method was designed and carried out according to that described by Kanekasu, et al. 2004 [14].
CT was carried out following each TKR to verify the rotation of the femoral component. The CT measurements were based upon the condylar twist angle (a line between the condylar and transepicondylar lines), and SEA (a line connecting the sulcus of the medial epicondyle with the prominence of the lateral epicondyle). The CT scans were conducted with the patient on a wooden table 70 cm high; this allowed for setting the x-ray lamp about 15° higher, in order to avoid soft tissue overlap on the final x-rays (Figure 1).
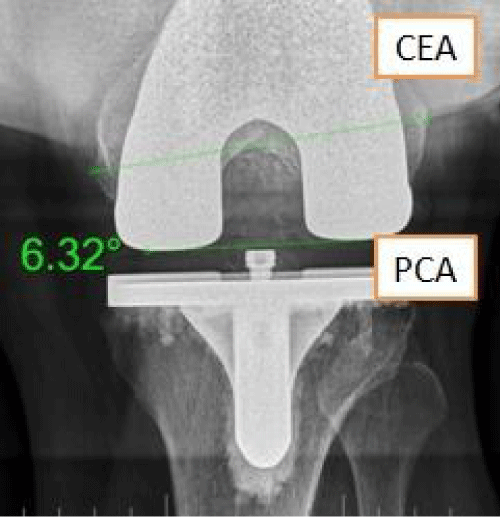
Figure 1: Flexion- relaxed X-ray of with the 15° of higher x-ray lamp, set to X-ray to miss the avoid soft tissue overlap. The clinical epicondylar axis (two values CEA) and posterior condylar axis (PCA) were measured to have determined the exact outer rotation of the femoral component FC of the total knee replacement TKR; here, the outer rotation was – here measured 6.32°.
On this 70-cm high wooden table, it was important to have the patient’s post-TKR knee in neutral rotation, to obtain resting x-rays. The position of the knee was then adjusted so that the central ray of the x-ray beam would be directed to the center of the patella. The distance between the x-ray tube and the film cassette was set at 100 cm. The obtained x-ray images were used to measure, first, the axis between the clinical epicondylar prominences and, second, the posterior condylar axis. These two axes form the middle twist angle. Ultimately, these data were compared to the related data in the literature to determine the failure data profile that when applied will allow for avoidance of failures in future implantations.
To assess the patients’ satisfaction with the clinical results after TKR, the Knee Society Score (also known as the KSS) was employed. The KSS was developed in 2011 as a patient-derived outcome measure to better characterize post-TKR satisfaction, expectations, and abilities for physical activities [15,16].
The average middle twist angle for all study participants was 3.36° (range: 1° - 7.6°). This result was similar to that in the literature. Our data presented herein is all for outer rotation. We prefer to perform the femoral sizing from the posterior upward, as this is most reliable for restoring the joint line in flexion, balancing the posterior cruciate ligament, and minimizing mid-flexion laxity. To create more external rotation, either the medial pinhole has to be moved upward or the lateral pinhole has to be moved downward.
The average KSS for all study participants was average 45% – 85%. Three patients gave KSS that corresponded to poor outcome (44.8%, 29% and 22%; Figure 2), x-rays showing discrepancy in flexion for the first two patients, respectively, are provided in figure 3. The third patient, with 22% KSS, showed no difference on the axial x-ray and was most probably generally unsatisfied with the TKR.
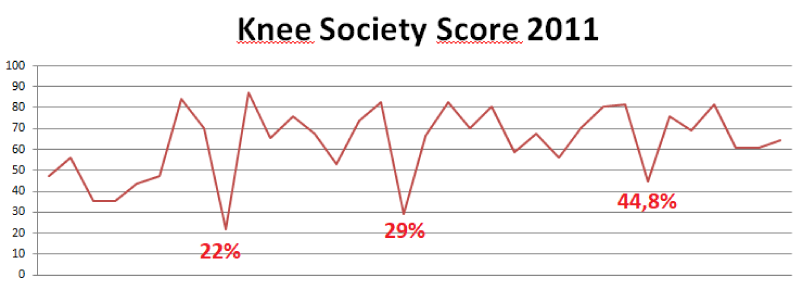
Figure 2: Knee Society Scores for the study population. The highest level of satisfaction was 87.4%, corresponding to excellent. The average range of KSS was 80 – 60%, corresponding to good-fair.
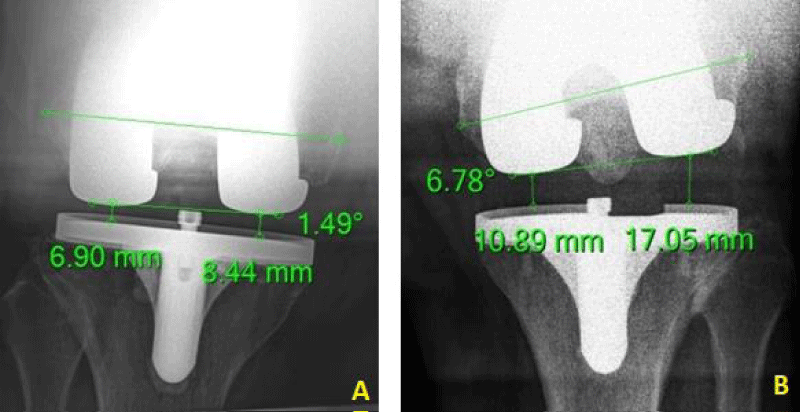
Figure 3: Axial flexion x-rays from the two patients whose Knee Society Scores indicated dissatisfaction after the TKR. The images show flexion-relaxed discrepancy (i.e. instability). A – a 79 year-old patient, with 29% Knee Society Score. B – a 70 year-old patient, with 44.8% Knee Society Score.
Four methods are available to select the right rotation of the femoral component during TKR in our hospital. The first usually involves choosing the rotation according to the Whiteside’s line (i.e. trans-sulcus line); this line should be constructed from the lowest part of the intercondylar sulcus to the intercondylar notch. The second involves the transepicondylar axis, which is parallel to the Whiteside line. The third involves the resection block oriented for the resections to be carried out at 3° outer rotation to the posterior condyles. The fourth method uses the tibial resection block, which is oriented parallel to the biomechanical limb axis. Applications of the four methods are presented in figure 4.
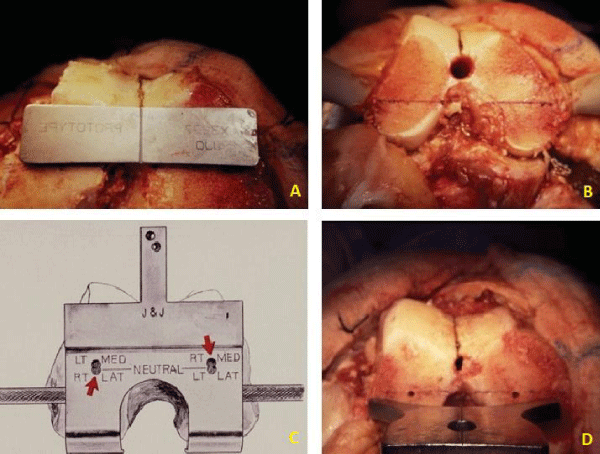
Figure 4: The four methods to obtain proper rotation of the femoral component in TKR. A – Representative intraoperative image of rotation made according to the Whiteside line (trans-sulcus axis). B – Representative intraoperative image of use of the transepicondylar axis (parallel to the Whiteside line). C – The resection block set to 3° outer rotation to the posterior condylar axis. D – Representative intraoperative image of use of the tibial resection block, parallel to the biomechanical limb axis. (Scott R.D., Total Knee Arthroplasty, Elsevier, 2006).
To balance a varus knee in flexion (having hyperplastic medial condyle of the femur), a greater degree is required to correct the flexion space. In a valgus knee, it is important to first balance in flexion and then in extension. The valgus deformity is usually caused by hypoplasia that is distal to and on the posterior part of the femur. For varus knees, the medial pinhole is almost always moved upward, to provide more medial space in flexion. For valgus knees, owing to the hypoplastic lateral femoral condyle, the lateral hole in usually moved downward.
It is rare for a knee to require internal rotation off the posterior condylar axis to achieve flexion gap symmetry; we can recommend such for only two types of cases. The first is a severe varus knee that has suffered erosion of the posterior medial femoral condyle. The second is a post-osteotomy knee that has the tibial joint line in excessive valgus axis. For good balance of the femoral popliteal joint, we use the reverse cruciform release to achieve full popliteal balance in extension. We seldom use the lateral collateral ligament release technique or the popliteal and biceps tendon release technique in flexion. For the most severe deformities that cannot be balanced, we use the constraint modular system.
Malrotation of a femoral component in TKR is a cause of persistent pain and poor function postoperatively. The malrotation has been reported to produce patellofemoral problems, flexion instability, ultra-high molecular weight polyethylene wear, stiffness, and abnormal patterns. The optimal setting of the femoral rotation is different for every knee. It should, however, always be in outer rotation of not more than 7°, to counter any worsened balance in the flexion space postoperatively. Inner rotation of the femoral component leads to malfunction of the femoro-patellar line, and eventually arthrofibrosis and lateral impingement. We recommend the application of Whiteside’s balancing of the flexion position of the femoral component in TKR, or use of the transepicondylar axis. Before operation, x-ray Kanekasu balancing can provide additional data to better balance the knee. Still, the development of other parameters for knee balance will provide important forensic value for patients who undergo TKR, improving operative success and individual satisfaction. Our recommendation to have good results in TKR is to do x-rays before and postoperatively. 3 views are essential: 1) antero-posterior, 2) lateral, and 3) Kanekasu projection to know the rotation after TKR. These projections seem to be basic to have good output of the TKR. Other cases without stability in flexion are nor very rarely planed for revision surgery, which is much more expensive, and burdens overall health system.
- Rodrics DJ, Patil P, Cowell Jr CW. Press-fit condaylar design total knee artroplasty. Fourteen to seventeen-year follow up. J Bone Joint Surg Am. 2007; 89: 89-95. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/17200315
- Hernandez-Vaquero D, Noriega-Fernandez A, Fernandez-Carreira JM, Fernandez-Simon JM, Llorens de los Rios J. Computer-assisted surgery improves rotational positioning of the femoral component but not the tibial component in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014; 22: 3127–3134. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/25155048
- Scott CE, Howie CR, MacDonald D, Biant LC. Predicting dissatisfaction following total knee replacement: a prospective study of 1217 patients. J Bone Joint Surg Br. 2010; 92: 1253–1258. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/20798443
- Lombardi Jr AV, Berend KR, Adams JB. Why knee replacements fail in 2013: patient, surgeon, or implant? Bone Joint J. 2014; 96-B(11 Supple A): 101–104. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/25381419
- Sharkey PF, Lichstein PM, Shen C, Tokarski AT, Parvizi J. Why are total knee arthroplasties failing today—has anything changed after 10 years? J Arthroplasty. 2014; 29: 1774–1778. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/25007726
- Franceschini V, Nodzo SR, Gonzalez Della Valle A. Femoral component rotation in total knee arthroplasty: a comparison between Transepicondylar Axis and posterior condylar line referencing. J Arthroplasty. 2016; 31: 2917–2921. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/27374639
- McDougall CJ, Gallie P, Whitehouse SL. Preoperative assessment of femoral rotation and its relationship with coronal alignment: a magnetic resonance imaging study. J Orthop. 2016; 13: 290–293. Y. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/27408506
- Victor J. Rotational alignment of the distal femur: a literature review. Orthop Traumatol Surg Res. 2009; 95: 365–372. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/19592323
- Howell SM, Papadopoulos S, Kuznik KT, Hull ML. Accurate alignment and high function after kinematically aligned TKA performed with generic instruments. Knee Surg Sports Traumatol Arthrosc. 2013; 21: 2271–2280. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/23948721
- Nam D, Lin KM, Howell SM, Hull ML. Femoral bone and cartilage wear is predictable at 0 degrees and 90 degrees in the osteoarthritic knee treated with total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2014; 22: 2975–2981. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/24839078
- Kobayashi H, Akamatsu Y, Kumagai K, Kusayama Y, Aratake M, et al. Is the surgical epicondylar axis the center of rotation in the osteoarthritic knee? J Arthroplasty. 2015; 30: 479–483. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/25466167
- Aunan E, Østergaard D, Meland A, Dalheim K, Sandvik L. A simple method for accurate rotational positioning of the femoral component in total knee arthroplasty. Acta Orthop. 2017; 11: 1–7. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/28799446
- Akagi M, Yamashita E, Nakagawa T, Asano T, Nakamura T. Relationship between frontal knee alignment and reference axes in the distal femur. Clin Orthop Relat Res. 2001; 388: 147–156. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/11451114
- Kanekasu K, Kondo M, Kadoya Y. Axial radiography of the distal femur to asses rotational alignment in total knee artroplasty. Clin Orthop Relat Res. 2004; 434: 193-197. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/15864052
- Noble PC, Scuderi GR, Brekke AC, Sikorskii A, Benjamin JB, et al. Development of a new Knee Society scoring system. Clin Orthop Relat Res. 2012; 470: 20-32. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/22065240
- Scuderi GR1, Bourne RB, Noble PC, Benjamin JB, Lonner JH, et al. The new Knee Society knee scoring system. Clin Orthop Relat Res. 2012; 470: 003-019. PubMed: https://www.ncbi.nlm.nih.gov/pubmed/22045067