Research Article
Administration of Non-Pharmachologic Intervention in the control of Hypertension among selected volunteer retirees in Awka Metropolis Anambra State Nigeria
Alagbu Chukwubuikem Eugene1*, Alagbu Chinwe Adline2, Chike Ijezie Ifeoma Blessing3 and Agwubike Elias Okey4
1Ph.D, Department of Human Kinetics and Health Education, Faculty of Education, Nnamdi Azikiwe University, Awka, Nigeria
2Department of Educational Management and Policy, Faculty of Education, Nnamdi Azikiwe University, Awka, Nigeria
3Department of Medicine and Surgery, Nnamdi Azikiwe University teaching hospital Nnewi, Nnewi Campus, Nigeria
4Department of Health Environmental and Human Kinetics, Faculty of Education, University of Benin, Benin City, Nigeria
*Address for Correspondence: Alagbu Chukwubuikem Eugene, Ph.D, Department of Human Kinetics and Health Education, Faculty of Education, Nnamdi Azikiwe University, Awka, Nigeria, Tel: +2348067968440; Email: [email protected]
Dates: Submitted: 20 October 2017; Approved: 03 November 2017; Published: 06 November 2017
How to cite this article: Eugene AC, Adline AC, Blessing CII, Okey AE. Administration of Non-Pharmachologic Intervention in the control of Hypertension among selected volunteer retirees in Awka Metropolis Anambra State Nigeria. J Sports Med Ther. 2017; 2: 129-137. DOI: 10.29328/journal.jsmt.1001018
Copyright License: © 2017 Eugene AC, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Non-pharmacologic; Prescription; Resting heart rate; Bicycle egometer; Essential hypertension; Systolic and diastolic blood pressure

Abstract
High blood pressure under medical palance is associated with a variety of circulatory diseases, and it has been estimated that over 12% of all deaths in the world is directly or remotely connected with hypertension. It is said that one out of every five persons, can expect to have high blood pressure at one time or the other, during one’s life time. Based on hemodynamic equation, the mean arterial pressure is equal to cardiac out-put, times resistance (p means=Q x R). Hence hypertension is usually as a result of either an increased cardiac output and/or an increased resistance. The most common form of high blood pressure in humans is called “essential hypertension”, while is said to have no known cause. However this research aims at showing how a 12-week moderate exercise with bicycle egometer (i.e., use of non-pharmacologic approach to reduce the resting heart rate and blood pressure of 6 volunteer retired civil servants from Anambra state civil service and 6 retired academic staff of Nnamdi Azikiwe university in Awka. The paired T-test analysis of data obtained revealed a statistical significant effect of the moderate 12-week exercise on bicycle egometer, on the resting heart rate and blood pressure of the experimental group of the respondents. Hence it could be concluded that the administration of moderate exercise on bicycle egometer could be an effective use of non-pharmacologic intervention in the control and prevention of high blood pressure or hypertension among the elderly.
Introduction
High blood pressure or hypertension refers to both systolic and diastolic blood pressures of an individual being above the normal level [1]. According to Owolabi, Owolabi, Olaolorun and Amole (2014), systolic blood pressure (SBO) of ≥140 mmHg, and diastolic blood pressure (DBP) of ≥90 mmHg in adults between the ages of 18 and above are regarded as the normal. Hence hypertension could be defined as the persistent or continuous elevation of blood pressure above this stated range. The inherent dangers associated with this ailment or health condition is that, majority of the victims are unaware of their being hypertensive, due to the fact that, usually there may be no visible or observable signs and symptoms of its presence, especially when it may not have caused any noticeable damage on any of the target organs e.g. the heart, kidney, liver, eye, or brain. Hence the disease is nicknamed, “Silent Killer”. However through verifiable researches, there are some clinical manifestations that can serve as clues to an individual to suspect the presence of hypertension.
They include:-
1. Severe and persistent occipital headache especially at the early hours of the day.
2. Blurred vision, dizziness, sleeplessness and uncommon chest pain (Elshamy 2012).
It is noteworthy however, that mere noticing or the observation of the above listed symptoms alone cannot be sufficient proof or evidence that such an individual is hypertensive. Inorder to establish any case of hypertension, requires a comprehensive diagnosis and examination by a clinician many times, over a period of time, before finally an individual could be declared hypertensive.
Hypertension as follows: (Figure)
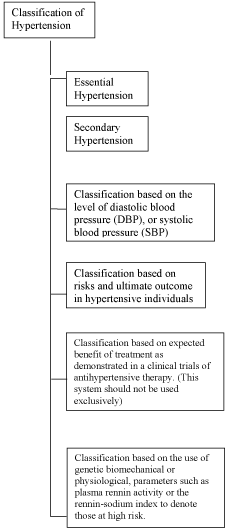
Figure :
The above classifications are useful to clinicians by providing them facts about when hypertension begins, which equally helps in their assessment of levels of risk, determination of prognosis and guide to therapeutic management of the ailment (Department of Preventive Medicine, Rush-Presbyterian-St. Luke’s medical Center, Rush Medical College of Rush university Chicago III, 1996).
According to Marshal [2], factors that may pre-dispose an individual to hypertension include:-life style of an individual, the family history, age of an individual, race and gender. The life style of an individual is the most critically cited pre-disposing factor, since it encompasses smoking habits, alcoholic dependence, drug use and abuse, excessive intake of table salt, overeating habit and lack of physical exercises (sedentary job/living habit).
Even though family history has been equally persistently pointed as a possible predisposing factor to hypertension, however when an individual knows that hypertension runs in their family linage and departs from the known pattern of living/eating habit of the family, such an individual may not likely develop the ailment. Hence according to American Heart Association [3], (AHA) averred that when life-style is considered as predisposing factor to the on-set of hypertension it is necessary to describe it further, as modifiable factor as against the non-modifiable ones, such as age and gender.
According to [2] Marshal the elderly people are more likely to become hypertensive than younger ones. Through researches it has also been proved, that male individuals start being hypertensive from the age of 54 and above, while females are likely to start experiencing hypertension from later age of 65 and above.
In this research study despite the fact that there are numerous other moderate physical exercises that could help to control or manage a hypertensive condition, however the researchers decided to use the bicycle egomenter which is easy to use, when compared with the treadmill or the elliptical gym machines. The bicycle egometer is an exercise equipment for novices in sports activates, including the elderly with back, knee and joint problems, that make running or brisk walking difficult. The equipment can be used both indoors and outdoors, hence the user doesn’t have to worry about inclement weather conditions or paying to belong to a commercial gym club. The bicycle egometer is a good alternative to the trade mill for the elderly individuals who have orthopeadic peripheral vascular or neurological limitations, that restrict weight bearing exercises. It is also less expensive, than most other gym equipment for physical exercises.
The bicycle egometer is a stationary bicycle with dynamometer which measures the strength of an individual’s muscles contraction. There are many different types of bicycle ergometers such as:
Ergometer Exercise bike ERG 9105 plus
ERG 9115 plus
BIKE FORMA (Technogym)
Run – 700/T
Run – 14 00/T
Run – 7409/T
Semi- Recumbent Egometer Exercise Bike
Run-7412/T
Em-7409
CMVC 10
XR50
XR 100
XR 100 NIBP (Cadidine)
Semi-Recumbent Ergometer Exercise Bike (√)
Ergoselect 600
Ergoselect 400
Torqualizer 600-Med
Ergometer Exercise Bike
Eurobike 3200 (LUMED
Eurobike 4200 (LUMED)
Sana 320F (Egosana)
Sana 350F (Egosana)
Sana 450 F (Egosana)
Sana comfort (Egosana)
Ergometer Exercise Bike
Ergoselect 4
Ergoselect 5 (Just to mention a few)
There are various ways of measuring high blood pressure, according to Chobonain, Bakris Black, Custman, Greece [4], they listed the following as the different places blood pressure could be measured using different devices, because they believed that the place where blood pressure is measured determines the type, device and method to be used. Hence, they averred that there is office blood pressure measurement. This is the type done in doctors consulting room, which involves the use of mercury device and stethoscope. Its short-coming is what is referred to as the “white coat effect”.
The ambulatory blood pressure monitoring (ABPM) In this type, blood pressure is monitored for 24 hours during the day and during sleep, using electronic device that senses arterial waves which the patient wears as arm band. Home blood pressure monitoring (HBPM) in this blood pressure assessment is a practical approach to assess the indidivual’s blood pressure while at home as against the work place. The self-blood pressure monitoring or the aneroid or electronic device could be used. In the case of this research, the instruments used for the recording of the initial and subsequent blood pressures of the respondents were the stethoscope and stop watch. The stethoscope manufactured by med. Laboratory England in 1990 and stop watch manufactured by Aronca in 1986, to monitor resting heart rate of the respondents. While the “Ergometer Exercise Bike ERG 9105 plus was used for the exercise experiment.
According to WHO (2013) the various ways of managing hypertension include choice of healthy diet, physical exercises avoidance of alcohol intake, relaxation therapy and avoidance of caffeine/hard drugs. However, this research is set to ascertain the effect of the use of physical exercise (non-pharmacologic means) (bicycle egometer) as exercise instrument in the control of hypertension among selected volunteer retirees in Awka metropolis Anambra State Nigeria.
Methodology
The researcher was able to acquire the 6 bicycle egometers used for the study by working in collaboration with a distributor-agent of gymnastic equipment out-fit in Awka metropolis. The deal was that the research study would serve as a medium to advertise bicycle egometers as instrument for physical exercise, and promote sales for the dealer, while the researcher benefits from the scientific result of the research study and contribution to knowledge. All the 12 volunteers before the commencement of the research study were subjected to clinical examination by a physician to certify them fit to participate in the study. Furthermore, the participants were made to sign an “informed consent form” and willingly agreeing to participate in the research study, however, without knowing who was to be in the control or experimental group. The participants were made to report to the venue of the exercise which was a small separate reception hall in a newly built hotel in the neighborhood, freely offered to the researcher for the period of the study, on Mondays, Wednesdays and Fridays from 7-10am, for the 12 weeks.
On arrival, the first day of the exercise, the participants were made to sit and rest for 10 minutes. After which the researcher presented them with 12 folded pieces of paper, out of which 6 of them were inscribed “CG meaning control Group” while the other 6 pieces had “EG” inscribed on them meaning experimental group. The 6 candidates that picked the papers with the inscription “EG” were the ones used for the experiment, while the others that picked CG served as the control group. On each of the days used for the research work, those in the experimental group were made to warm up for 10-15 minutes which involved walking around and stretching exercise, before getting on the bicycle egometer for a 30 minutes ride, while those in control group were made to sit down on provided plastic chairs to watch, those in the experimental group.
During the first 4 weeks all the bicycle egometers were adjusted in such a way that peddling was easy. The adjustments were systematically increased during the remaining 2nd, 3rd and four weeks respectively, which increased the work load for the participants. At the end of every 30 minutes work-out, an interval of 5 minutes was allowed for cool down. At this point, the heart rates of those in the experimental group were again measured and recorded for use in the computation, as past intervention resting heart rate. Equally the resting heart rate of those in the control group were also measured and recorded and used as control groups post non-intervention resting heart rate.
Data analysis
Results/Findings: The variables studied are hereunder presented showing their means, standard deviation and the range of measurements (their minimum and maximum rates, both for the experimental and the control groups (Tables 1,2).
| Table 1: Descriptive analysis of the variables studied in the experimental Group (A). | |||||
| Variables | N | Min | Max | Mean | STD Deviation |
| Pre -Experimental systolic blood pressure | 6 | 145.00 | 190.00 | 168.3333 | 15.0555 |
| Pre- Experimental diastolic blood pressure | 6 | 95.00 | 105.00 | 98.3333 | 4.0825 |
| Pre -Experimental Resting Heart Rate | 6 | 90.00 | 120.00 | 102.5000 | 10.8397 |
| Post -Experimental systolic blood pressure | 6 | 130.00 | 160.00 | 145.0000 | 10.0000 |
| Post -Experimental diastolic blood pressure | 6 | 85.00 | 95.00 | 89.1667 | 3.7639 |
| Post -Experimental Resting Heart Rate | 6 | 60.00 | 85.00 | 72.5000 | 9.3541 |
| Valid N (Listwise) | 6 | ||||
| Table 2: Descriptive analysis of the variables studied in the experimental Group (A). | |||||
| Variables | N | Min | Max | Mean | STD Deviation |
| Pre -Experimental systolic blood pressure | 6 | 150.00 | 180.00 | 163.3333 | 10.8012 |
| Pre- Experimental diastolic blood pressure | 6 | 95.00 | 105.00 | 98.3333 | 4.0825 |
| Pre -Experimental Resting Heart Rate | 6 | 90.00 | 120.00 | 104.1667 | 11.1430 |
| Post -Experimental systolic blood pressure | 6 | 155.00 | 175.00 | 163.333 | 6.8313 |
| Post -Experimental diastolic blood pressure | 6 | 90.00 | 100.00 | 96.6667 | 4.0825 |
| Post -Experimental Resting Heart Rate | 6 | 90.00 | 110.00 | 98.3333 | 6.8313 |
| Valid N (Listwise) | 6 | ||||
Comparative analysis of data
Presented in table 3 is the statistical sample pairings of the various variables studied in this research. The purpose of these pairing is to show the comparison of the values of the variables studied, both in the experimental group (A) and the control Group (B), before and after the 12 weeks exercise on the bicycle egometer as a non-pharmacologic intervention in the control of hypertension in the elderly.
| Table 3: Paired Samples Statistics of the Variables. | |||||
| Pairs | Variables | Mean | N | Std Deviation | Std. Error Mean |
| Pair 1 | A’s Pre-Experimental Systolic Blood Pressure | 168.3333 | 6 | 15.0555 | 6.1464 |
| A’s Post-Experimental Systolic Blood Pressure | 145.0000 | 6 | 10.0000 | 4.0825 | |
| Pair 2 | B’s Pre-Experimental Systolic Blood Pressure(Control) | 163.3333 | 6 | 10.8012 | 4.4096 |
| B’s Post-Experimental Systolic Blood Pressure(Control) | 163.3333 | 6 | 6.8313 | 2.7889 | |
| Pair 3 | A’s Pre-Experimental Diastolic Blood Pressure | 98..3333 | 6 | 4.0825 | 1.6667 |
| A’s Post-Experimental Diastolic Blood Pressure | 89.1667 | 6 | 3.7639 | 1.5366 | |
| Pair 4 | B’s Pre-Experimental Diastolic Blood Pressure(Control) | 97.5000 | 6 | 2.7386 | 1.1180 |
| B’s Post-Experimental Diastolic Blood Pressure(Control) | 98.3333 | 6 | 4.0825 | 1.6667 | |
| Pair 5 | A’s Pre-Experimental Resting Heart Rate | 102.5000 | 6 | 10.8397 | 4.4253 |
| A’s Post-Experimental Resting Heart Rate | 72.5000 | 6 | 9.3541 | 3.8188 | |
| Pair 6 | B’s Pre-Experimental Resting Heart Rate(Control) | 104.1667 | 6 | 11.1430 | 4.5491 |
| B’s Post-Experimental Resting Heart Rate(Control) | 98.3333 | 6 | 6.8313 | 2.7889 | |
| Pair 7 | A’s Pre-Experimental Systolic Blood Pressure | 168.3333 | 6 | 15.0555 | 6.1464 |
| B’s Pre-Experimental Systolic Blood Pressure(Control) | 163.3333 | 6 | 10.8012 | 4.4096 | |
| Pair 8 | A’s Pre-Experimental Diastolic Blood Pressure | 98.3333 | 6 | 4.0825 | 1.6667 |
| B’s Pre-Experimental Diastolic Blood Pressure(Control) | 97.5000 | 6 | 2.7386. | 1.1180 | |
| Pair 9 | A’s Pre-Experimental Resting Heart Rate | 102.5000 | 6 | 10.8397 | 4.4253 |
| B’s Pre-Experimental Resting Heart Rate (Control) | 104.1667 | 6 | 11.1430 | 4.5491 | |
| Pair 10 | A’s Post-Experimental Systolic Blood Pressure | 145.0000 | 6 | 10.0000 | 4.0825 |
| B’s Post-Experimental Systolic Blood Pressure (Control) | 165.3333 | 6 | 6.8313 | 2.7889 | |
| Pair 11 | A’s Post-Experimental Diastolic Blood Pressure | 89.1667 | 6 | 3.7639 | 1.5366 |
| B’s Post-Experimental Diastolic Blood Pressure (Control) | 98.3333 | 6 | 4.0825 | 1.6667 | |
| Pair 12 | A’s Post-Experimental Resting Heart Rate | 72.5000 | 6 | 9.3541 | 3.8188 |
| B’s Post-Experimental Resting Heart Rate (Control) | 98.3333 | 6 | 6.8313 | 2.7889 | |
Discussion
According to Halbert, Silagy, Finucane Witheers, Hamdorf and Andrews [5], resistance exercises are not suitable in reducing high blood pressure, rather the aerobic exercises shows a more significant clinical effect in the reduction of Systolic Blood Pressure (SBP) and Diastolic Blood Pressure (DBP). In this regard Insel and Roth [6], National heart and Blood Institute [7,8], (NHLBI) revealed from their studies that aerobic exercises directly interferes with disease processes that cause coronary artery blockage and enhances the functions of the cells that line the arteries, thereby making blood flow easy. Furthermore Jimoh [9], reported that aerobic (dynamic exercises), which involves steady and constant motion of the muscles, increases the body demand for oxygen and makes the muscles of the heart healthier. Similarly Adefuye and Akeredolu [10], reported that a two week regular exercise programme is beneficial in patients with high blood pressure and concluded that exercise in black individuals resulted in significant reduction of systematic blood pressure.
Furthermore in support of the earlier views of experts on the suitability of specific types of exercises for control and prevention of high blood pressure, Kravitz [11], cautioned that not all physical activities are suitable for lowering blood pressure, since the evidence is not as supportive on the effectiveness of resistance training in lowering blood pressure. In line with the views of these experts Alagbu, Alagbu and Agwubike [12], averred that aerobic exercises which engages large groups of muscles continuously for over 15 minutes or more raises the heart rate, breathing rate and body temperature, a consideration that gives credence to the present study of using bicycle egometer in the control of hypertension in elderly retirees in Anambra state.
In deed the use of bicycle egometer in this study has proved to be ideal aerobic exercise, suitable for controlling or preventing hypertension among the elderly. This claim could be supported by the finding of this research as shown in table 3, where the systolic/diastolic blood pressures and resting heart rates values of pairs 1, 3 and 5 of the respondents in the experimental group at the beginning of the exercise programme were paired for comparison, with the values of the same variables at the end. The paired t-test analysis of these pairs showed in table 4, resulted to the following t-values with the corresponding 2-tailed significance level.
| Table 4: Paired Samples T-Test Results Paired Differences. | ||||||||
| Mean | STD Deviation | Std Error Mean | 95% Confidence interval of the Difference | |||||
| Lower limit | Upper limit | t | df | Sig. Z-tailed | ||||
| Pair 1 | 23.3333 | 16.3299 | 6.6667 | 6.1961 | 40.4705 | 3.500 | 5 | 0.017 |
| Pair 2 | 0.0000 | 5.4772 | 2.2361 | -5.7480 | 5.7480 | 0.000 | 5 | 1.000 |
| Pair 3 | 9.1667 | 3.7639 | 1.5366 | 5.2167 | 13.1166 | 5.966 | 5 | 0.002 |
| Pair 4 | -8333 | 5.8452 | 2.3863 | -6.9675 | 5.3009 | -0.349 | 5 | 0.741 |
| Pair 5 | 30.0000 | 17.8885 | 7.3030 | 11.2271 | 48.7729 | 4.108 | 5 | 0.009 |
| Pair 6 | 5.8333 | 12.4164 | 5.0690 | -7.1969 | 18.8635 | 1.151 | 5 | 0.302 |
| Pair 7 | 5.0000 | 11.4018 | 4.6547 | -6.9654 | 16.9654 | 1.074 | 5 | 0.332 |
| Pair 8 | .8333 | 5.8452 | 2.3863 | -5.3009 | 6.9675 | 0.349 | 5 | 0.741 |
| Pair 9 | -1.6667 | 6.8313 | 2.7889 | -8.8357 | 5.5023 | -.598 | 5 | 0.576 |
| Pair 10 | -18.3333 | 13.2916 | 5.4263 | -32.2820 | -4.3847 | -3.379 | 5 | 0.020 |
| Pair 11 | -9.1667 | 6.6458 | 2.7131 | 16.1410 | -2.1923 | -3.379 | 5 | 0.020 |
| Pair 12 | -25.8333 | 13.9344 | 5.6887 | -40.4566 | -11.2101 | -4.541 | 5 | 0.006 |
Pair 1 t=3.5 sig. (2-tailed)=0.017
Pair 3, t=5.966, sig (2-tailed)=0.002, while
Pair 5, t=4.108, sig (2-tailed)=0.009
These computed t-values have 2-tailed significant levels which are less than the 0.5 significance level set for this research study.
The difference between the pre-test and post-test systolic/diastolic blood pressure and resting heart rates are therefore significant.
Based on the above result, the 12 week exercise administered on the respondents using bicycle egometer (experimental group) (retirees) significantly lowered their systolic/diastolic and resting heart rates respectively.
In order to rule out the chances of other factors being responsible for these observed systolic/diastolic blood pressure and resting heart rates of the respondents in the experimental group, a pre-test and post-test values of the systolic/diastolic blood pressures and resting heart rates of the respondents in the control group were exhibited in pairs 2, 4 and 6 for analytical comparison, as displayed in table 4.
Here in table 4, the comparative t-test analysis revealed a no significant difference, in the control group’s systolic/diastolic blood pressure and resting heart rate values of those respondents, as at the beginning and end of the 12 weeks period. Hence, pairs 2, 4 and 6 show a computed t-values of 0.000, -0.349 and 1.151 individually, with 2-tailed significance levels of 1.000, 0.741 and 0.302 respectively. Since, these significant levels are all higher than the 0.05 level of significance set for this research study. Invariably, this scenario depicts a no significant difference in the control group’s systolic/diastolic blood pressures and resting heart rates comparatively at the beginning and the end of the 12 weeks period.
It is vital to note that all the volunteers who opted to participate in the research study (those in the experimental and control groups, had so many similarities, before the commencement of the research, for example, they all reside in the same neighborhood, where there are virtually no recreational facilities, like tennis courts, basketball courts and swimming pools, they all were retirees lecturers or civil servants, nearly all of them patronize private medical clinics in the neighborhood for their occasional high blood pressure checks and treatment, finally, none of the participants had earlier before the study been using bicycle egometer as exercise equipment, and they were all males. Hence, their pre-experimental systolic/diastolic blood pressure and resting heart rates were not significantly different as depicted in the paired t-test analysis of pairs 7, 8 and 9 as shown in table 4.
Since all the participants reported to the venue of the research study every Mondays, Wednessdays and Fridays of each week for the purpose of the research in their cars, and were subjected to virtually same condition in all such days, invariably the differences observed in the post-experimental blood pressure and resting heart rates effect observed among the experimental group, was as a result of the exercise administered on them with the bicycle egometer.
The result of this research study therefore is consistently in support of Kravitz [11], who asserted that aerobic exercises lowers blood pressure by reducing the blood level of norpinephrine which in turn limits the vasoconstriction of the arterioles thereby resulting to less peripheral resistance to blood flow, furthermore, brings about increase in the parasympathetic activity and a decrease in sympathetic discharge in the nervous system which leads to a lowered resting heart rate in an individual, all of which culminates to reduction of high blood pressure (hypertension).
In similar vein, the result of this study corroborates the findings of Alagbu, Alagbu and Agwubike [12], who stated that aerobic exercises which engages large groups of muscles of the human body continuously for over 15 minutes or more raises the heart rate, breathing rate, and body temperature which further helps to reduce insulin resistance and maintains insulin levels in an individual’s blood, which is essential in the reduction of hypertension.
Conclusion
Based on the findings of this study, it has been further shown that adequately administered moderate exercises with the bicycle egometer, following the due process as contained in the methodology of this research, could safely serve as non-pharmacologic intervention in the control of hypertension and equally as a therapy. This claim could be substantiated by the fact that the administration of exercises with the bicycle egometer on the experimental group of elderly retirees, who volunteered to participate in the research work had definite reduction in their systolic/diastolic blood pressure and resting heart rate, as clearly shown through the analysis of the data collected from the readings during the research study.
This study must have therefore contributed to the knowledge, that exercise adequately prescribed and administered, using the bicycle egometer, serves as an alternative therapeutic means of controlling the “dreadful monster hypertension”, which the use of drugs to cure over the years had sometimes resulted to other side effects or complications in a victim.
Recommendations
Based on the conclusion of the study it is therefore being recommended as follows:
1. That a similar research be conducted using all female retirees, since all the respondents in this research were all males.
2. Government should as a matter of policy when mapping out layouts and estates reserve sizable portions of open spaces for the construction of recreational facilities for the use of the inhabitants of such layouts/estates.
3. Government should in the same way ensure that regular checks are made to fish out quacks from other professions, same should be done for operators of exercise gym out-fits scattered over the country to ensure they are manned or operated by qualified experts in exercise prescription and administration under the supervision of qualified physicians.
References
- Herbert W. Risk factors of Essential hypertension. 2008. Ref.: https://goo.gl/TBBwC3
- Marshal K. Definition hypertension. 2008.
- American Heart Association (AHA). Understanding and managing High blood Pressure. 2014.
- Chobanian AV, Bakris GL, Black HR, Custman WC, Green LA, et al. JNC 7-complete version-Seventh report of the Joint national Conference Committee on Prevention, Detection and Evaluation and Treatment of High blood pressure. CiteSeer. 2003. Ref.: https://goo.gl/8aXWqT
- Halbert JA, Silagy CA, Funucane P, Withers RT, Hamdorf PA, et al. The effectiveness of excersice training in lowering blood pressure a meta-analysis of randomized controlled trials of 4 weeks of longer. Journal of Human Hypertension. 1997. Ref.: https://goo.gl/PHYNLC
- Insel PM, Roth WT. Come concepts in health. New York; McGraw Hill. 2000.
- National Heart Luna and Blood Institute (NHLBI). Lowering your Blood Pressure with a DASH. 2003.
- National Heart Luna and Blood Institute (NHLBI). Lowering your Blood Pressure with a DASH. 2006.
- Jimoh A. Get as fit as a fiddle. The Guardian Newspaper. 2000.
- Adefuye MA, Akeredolu OA. Quality of life of hypertensive patient. Journal of International Council for health, physical Education Recreation, Sports and Dance 2006; 1: 1-4.
- Kravitz L. Exploring the mysteries of exercise. 2007.
- Alagbu CE, Alagbu CA, Agwubike EO. Perception of exercise as psychogenic aids in the improvement of cardiovascular health: Implications to sports administration among young academic staff of Unizik Awka. Int J Sciences. 2013; 2: 32-36. Ref.: https://goo.gl/nLYdSP
- Owolabi AO, Owolabi MO, Olaolurun AD, Amole IO. Hypertension prevalence among a health workforce in Nigeria. 2014.
- WHO. WHO technical meeting on sleep and health. 2004.
- WHO. Clinical guidelines for the management of hypertension. 2005