Case Report
Seroma formation as a rare complication of lateral epicondylitis release: A case report
Parth B Patel1, Allison L Boden2*, Bryan J Sirmon2, Spero G Karas2 and Michael B Gottschalk2
1Morehouse School of Medicine, Atlanta, GA, USA
2Department of Orthopaedics, Emory University School of Medicine, Atlanta, GA, USA
*Address for Correspondence: Allison L Boden, Department of Orthopaedics, Emory University School of Medicine, Atlanta, GA, USA, Email: [email protected]; [email protected]
Dates: Submitted: 20 October 2017; Approved: 26 October 2017; Published: 27 October 2017
How to cite this article: Patel PB, Boden AL Sirmon BJ, Karas SG, Gottschalk MB. Seroma formation as a rare complication of lateral epicondylitis release: A case report. J Sports Med Ther. 2017; 2: 118-122. DOI: 10.29328/journal.jsmt.1001016
Copyright License: © 2017 Patel PB, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Abstract
Case: A 45 year old male, >1 year status post left elbow lateral debridement for lateral epicondylitis, presented with a two week history of a progressive, tender mass on the lateral aspect of his left elbow. MRI showed evidence of a defect in the joint capsule, consistent with the formation of a seroma. The patient underwent revision of the left lateral epicondyle debridement with ECRL/EDC tendon repair and capsular reconstruction.
Conclusion: Tendon repair and capsular reconstruction is an effective and successful method for the treatment of a seroma caused by leakage of joint fluid after lateral epicondylar debridement.
Introduction
Lateral epicondylitis, commonly referred to as “tennis elbow”, affects 1-3% of adults in the United States each year [1]. While a variety of treatment options exist, the majority of patients with this condition undergo conservative treatment prior to considering surgery, and approximately 90% of patients with lateral epicondylitis are treated successfully through non-operative methods [2]. Fortunately, patients that have recurrent or refractory symptoms are able to undergo lateral epicondylar release, excision, or repair of the common extensor tendon; these procedures reliably produce good results with very few reported complications. One study identified 67 articles that reported complications after lateral epicondylar release and found an overall complication rate of 3.3% [3]. One uncommon complication associated with this procedure is the formation of a seroma from leakage of joint fluid [3]. There is very little published on this rare complication and there are no reports of this complication occurring outside of the early-postoperative period. Because this is a rare complication that has not previously been described, this report presents the identification and surgical treatment of a seroma in a patient more than one year following lateral epicondylar debridement.
Case Report
The patient was a forty-five year old left hand dominant male, >1 year status post left elbow lateral epicondyle debridement at an outside hospital, who presented to a clinic with a progressive two week history of a tender mass on the lateral aspect of his left elbow. At the time of presentation, the patient had full range of motion at the elbow and was believed to have bursitis. Clear, yellow fluid was aspirated from the mass with no evidence of infection or gout. Inflammatory markers such as Rheumatoid Factor, anti-CCP, and Anti Nuclear Antibody were not investigated at this time, as there was low suspicion for inflammatory joint pathology; however, this is a limitation to this study. The patient returned one week later due to re-accumulation of the fluid, at which point he underwent a subsequent aspiration and was referred to our clinic for surgical consultation. Subsequent MRI of the elbow demonstrated a defect in the elbow joint capsule on the lateral aspect with an effusion communicating with a contiguous fluid collection along the posterolateral aspect of the elbow, consistent with a left elbow seroma (Figure 1). Conservative versus surgical options were discussed with the patient and the patient decided to proceed with surgery after informed consent was obtained. Preoperatively, the patient’s visual analog score (VAS) was 5 and his Quick Disabilities of the Arm, Shoulder, and Hand Score (QuickDASH) was 13.6. Of note, the patient reported that he did not have complete resolution of his pain after the index procedure.

Figure 1: Pre-operative axial, coronal, and sagittal T2 weighted magnetic resonance images of the patient elbow showing a defect in the elbow joint capsule on the lateral aspect with an effusion communicating with a contiguous fluid collection along the posterolateral aspect of the elbow.
Revision of the left lateral epicondyle debridement with extensor carpi radialis longus (ECRL) and extensor digitorum communis (EDC) tendon repair and capsular reconstruction was performed. The patient was brought to the operating room and placed in the supine position (Figure 2). A high arm tourniquet was then placed and the patient was given two grams of cefazolin. The patient’s prior incision was re-used and the skin was incised with a #15 blade under loupe magnification. The epidermis and dermis were opened and the lateral capsular structure was then identified, incised, and found to be confluent with the joint (Figure 3). A large amount of fluid was drained and sent for culture. The patient was examined for posterolateral rotatory instability, which the patient did not have; had this been present, the lateral radial collateral or annular ligament would have been reconstructed. Next, the extensor mass was inspected and we observed that the entire extensor carpi radialis brevis (ECRB) insertion and elbow capsule had been removed in the previous debridement; but, some portions of the ECRL and EDC remained intact. The synovial film was debrided and excised sharply with a scalpel and rongeur. The lateral epicondyle was then inspected and debrided with a rongeur. Care was taken to not debride too much of the ECRL and EDC, and a suture anchor was placed in the lateral epicondyle in order to hold the extensor mass and graft to the bone. The suture anchor was placed under fluoroscopic guidance to ensure proper placement. Given the size of the defect and the amount of scarring present, we did not feel as though the tissues could be mobilized enough to perform an anconeus flap. The joint was copiously irrigated, after which a GraftJacket (Wright Medical Technology, Arlington, TN) was sewn tightly into the ECRL/EDC and the lateral epicondyle (Figure 4). Running locking stitches were placed to seal the elbow joint. Once complete, we determined that the elbow was able to undergo full range of motion and fibrin glue was placed to act as a secondary seal of the joint. The subcutaneous fascia, dermis, and epidermis were closed and the patient was placed in cast padding and a long arm splint.

Figure 2: External landmarks were identified and marked prior to making an incision through the epidermis and dermis.
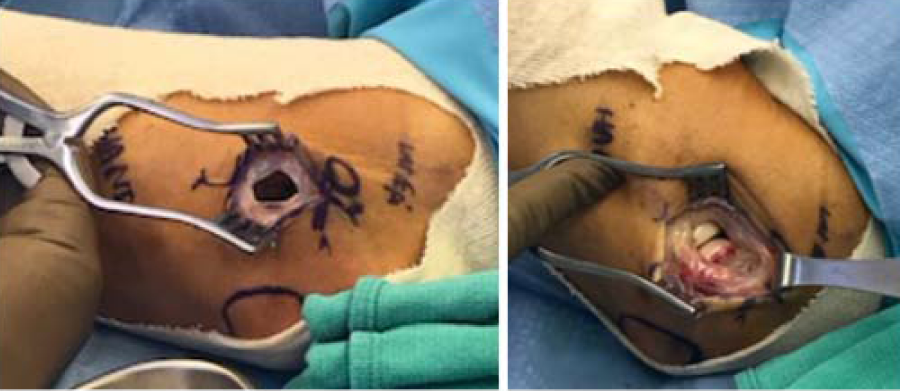
Figure 3: After making the incision through the previous scar, the lateral capsular structure was identified, incised, and found to be confluent with the joint.

Figure 4: A GraftJacket was sewn tightly into the ECRL/EDC and the lateral epicondyle and running locking stitches were placed to seal the elbow joint.
At the patient’s two week post-operative visit, the splint was removed and the patient was cleared to begin gentle range of motion exercises, with extra care taken for extension and flexion of the elbow and no weightlifting with the upper extremity. Five weeks after the revision surgery, the patient reported he was doing “extremely well” and had no pain at that time. Eight weeks status post revision surgery, the patient had full digital, wrist, elbow and shoulder range of motion, was neurologically intact, and there was no evidence of fluid re-accumulation (Figure 5). At this time, verbal consent was obtained to use his pictures and clinical data for a case report. Pain and functional outcomes were assessed nine months postoperatively, at which point the patient’s VAS was 0 and his QuickDASH was 4.5.
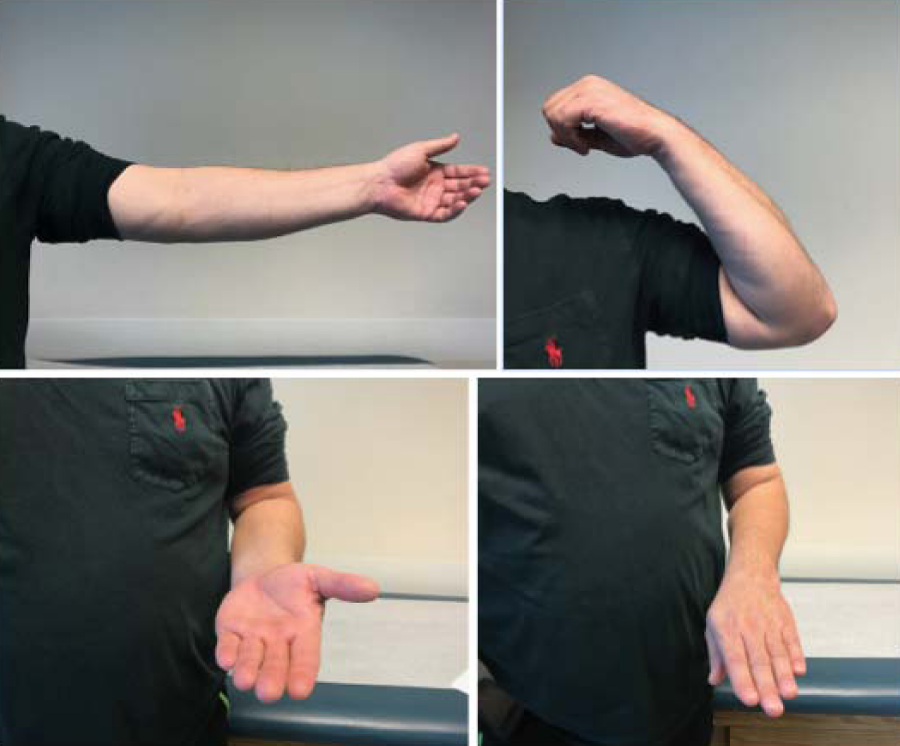
Figure 5: Eight weeks after the revision surgery, the patient had full range of motion at the elbow joint, including extension, flexion, supination, and pronation.
Discussion
While only 10% of patients who experience lateral epicondylitis require surgical intervention, it is important to understand what complications can arise from a lateral epicondylar release and how to manage them. The most frequent complications include nerve damage, wound issues, and infection [3]. A less common complication is seroma formation from leakage of joint fluid. To our knowledge, this is the first case report on the management of a delayed seroma following lateral epicondylar debridement.
An open procedure like this patient’s initial debridement is known to have higher complication rates than arthroscopic and percutaneous procedures [3]. The etiology of most seromas remains largely unknown; however, defects in anatomical joint capsule structures or iatrogenic defects acquired during surgical intervention are believed to contribute to their formation. In the case reported here, there were obvious structural abnormalities noted in the elbow joint capsule that we believe may have been iatrogenically created during the patient’s surgery more than a year prior. While highly unlikely, it is possible that a capsular defect was present prior to the initial procedure on the left elbow; we were unable to obtain previous radiographs for review.
While seroma formation from the leakage of joint fluid is a rare occurrence, there have been some reports of this occurring in the immediate post-operative period in patients treated for lateral epicondylitis. One study investigating outcomes after dis-insertion of the proximal tendon for lateral tendinopathy reported 1 seroma complication out of the 405 patients in the study; however, management of the complication was not described [4]. Cho et al., reported seroma formation in patients who underwent a mini-open muscle resection for lateral and medial epicondylitis [5]. Of the 42 patients who underwent the resection, 2 developed a seroma with leakage of joint fluid in the subcutaneous space that was noticed after suture removal [5]. Both patients were managed with an additional surgery in which the fluid was suctioned and a drain was placed [5].
Of the patients who developed seromas in the studies noted above, there was no report of pain and functional outcomes after the management of the seroma. Because this is the first reported case of delayed seroma formation, the patient’s postoperative pain and functional outcomes are important to note. The patient’s VAS score improved from 5 preoperatively to 0 at 9 months. Our patient’s QuickDASH score improved from 13.6 to 4.5, a difference of 9.1 points. The QuickDASH is scored on a scale from 0 to 100, with higher numbers indicting worse functional outcomes [6]. The minimal detectable change (MDC) has been shown to be 11 points on this scale [6]. While the patient’s improvement is close to but does not meet the MDC, the patient was “extremely satisfied” with the procedure overall and felt as though he was functioning at a higher level than before the procedure.
The lack of literature on this topic speaks to the infrequent nature of this complication. Assessing patients post-operatively for synovial or capsular damage via advance imaging is warranted if there are signs of fluid collection or a painful soft mass that develops after the procedure. In the event that capsular damage can be confirmed, we believe that capsular reconstruction is reasonable and effective as a treatment.
References
- Allander E. Prevalence, incidence, and remission rates of some common rheumatic diseases or syndromes. Scand J Rheumatol. 1974; 3: 145-153. Ref.: https://goo.gl/TKWaut
- Nirschl RP, Pettrone FA. Tennis elbow. The surgical treatment of lateral epicondylitis. J bone Jt Surg Am. 1979; 61: 832-839. Ref.: https://goo.gl/zx5GTA
- Pomerantz ML. Complications of Lateral Epicondylar Release. Orthop Clin North Am. 2016; 47: 445-469. Ref.: https://goo.gl/5rdNfu
- Cusco X, Alsina M, Seijas R, Ares O, Alvarez-Diaz P, et al. Proximal disinsertion of the common extensor tendon for lateral elbow tendinopathy. J Orthop Surg (Hong Kong). 2013; 21: 100-102. Ref.: https://goo.gl/aekUWK
- Cho BK, Kim YM, Kim DS, Choi ES, Shon HC, et al. Mini-open muscle resection procedure under local anesthesia for lateral and medial epicondylitis. Clin Orthop Surg. 2009; 1: 123-127. Ref.: https://goo.gl/tAstLu
- Polson K, Reid D, Mcnair PJ, Larmer P. Responsiveness, minimal importance difference and minimal detectable change scores of the shortened disability arm shoulder hand (QuickDASH) questionnaire. Man Ther. 2010; 15: 404-407. Ref.: https://goo.gl/Ctz6tF