Review Article
The role of UK national ligament registry as additional source of evidence for anterior cruciate ligament reconstruction: Review of the literature and future Perspectives
Tarek Boutefnouchet1,2*, Thomas Laios3 and Keshav Mathur4
1University Hospital Coventry and Warwickshire, Clifford bridge road, Walsgrave Coventry CV2 2DX, United Kingdom
2Warwick Medical School, the University of Warwick Coventry CV4 7AL, United Kingdom
3Department of trauma and orthopaedic surgery, Heart of England NHS Foundation Trust, Bordesley Green East, Birmingham B9 5SS, United Kingdom
4Alexandra Hospital, Worcester Acute Hospital NHS Trust, Woodrow drive Redditch B98 7UB, United Kingdom
*Address for Correspondence: Tarek Boutefnouchet, University Hospital Coventry and Warwickshire, Clifford bridge road Walsgrave, Coventry, CV2 2DX, United Kingdom, Tel: +44(0)7809677302; Email: [email protected]
Dates: Submitted: 16 August 2017; Approved: 29 August 2017; Published: 30 August 2017
How to cite this article: Boutefnouchet T, Laios T, Mathur K. The role of UK national ligament registry as additional source of evidence for anterior cruciate ligament reconstruction: Review of the literature and future Perspectives. J Sports Med Ther. 2017; 2: 081-090. DOI: 10.29328/journal.jsmt.1001012
Copyright License: © 2017 Boutefnouchet T, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Anterior cruciate ligament; Surgical management; Physiotherapy; Clinical decision-making; Clinical Registry; Cost-effectiveness

Abstract
Background: There is paucity in studies reporting long-term results following anterior cruciate ligament (ACL) rupture. A UK national ligament registry (NLR) designed to collect demographic, clinical and outcome data on patients undergoing ACL reconstruction was launched in 2013. There was therefore an emergent question on the role of such registry as an additional source of evidence.
Study aims: A framework analysis aimed to provide a basis for the evaluation of outcomes following ACL management and formulate a structure of the evidence, which can be derived from the registry.
Methods: A systematic approach was adopted to select relevant studies. Qualitative thematic and meta-narrative analyses were conducted. Level-1 registry data were recorded for all primary ACL reconstruction procedures from January to June 2016. Registry data content and validity were evaluated.
Results: Seven studies were suitable for analyses yet none defined the pattern of meniscal injury following initial treatment. When reported the incidence varied markedly between 23% and 80%. There was evidence of collection of at least one principal outcome measure in at least 85% of participants across all studies. Thematic analysis identified four key domains of outcome measures (1) intervention selection, (2) Knee stability evaluation, (3) Patient reported outcomes, (4) Radiographic evaluation and risk of secondary osteoarthritis. Graft choice, rate of meniscal and chondral injuries and cumulative risk of revision surgery had incomplete and inconsistent reports. Comparison of demographic and clinical data with the first registry report demonstrated: predominately younger patient population; older female patients at time of intervention; and higher incidence of meniscal tears.
Conclusions: Registry data driven quality and research improvement open a new paradigm in ACL reconstruction evidence base and future practice. Early observations have consolidated the importance of associated meniscal injuries in the management of ACL rupture. Further work is needed to improve registry data completeness, accuracy and validity. A proposed data migration process using available technologies can help harmonise data collection without the added burden on clinical services.
Introduction
Longitudinal prospective data collected in clinical registry contain specific clinical information on diagnosis and surgical procedures. A core component of any successful registry is a standardised data management approach and outcome reporting of a large scale. Lessons have already been learnt from well-established registries such as the National Joint Registry (NJR) on long-term outcomes related to implant survival and revision surgery. Similar to its predecessor the UK National Ligament Registry (NLR) has the potential to offer the ability to guide future clinical practice and health care policy.
Short to intermediate-term outcomes for both surgical reconstruction and structured rehabilitation treatments are well documented with Level-I and II evidence [1]. ACL reconstruction is utilized more commonly to facilitate return to sports and to protect the menisci and articular cartilage. Arguments for ACL reconstruction advocate prevention of instability, restoration of normal kinematics, and return to normal function and sports. Ultimately allowing joint preservation by preventing secondary meniscal lesions and degenerative changes, which can result from abnormal joint contact stresses [2-4]. In contrast, other authors reported satisfactory results and restoration of function with adequate rehabilitation. Structured rehabilitation is often reserved for lower-demand and older patients. Thus avoiding the risk of arthrofibrosis, graft impingement, graft failure, infection, and donor site morbidity [1,3,5,6]. Nordenvall et al concluded that ACLR had no protective effect against secondary osteoarthritis in the Swedish patient’s registry. This study however used solely secondary procedures as a surrogate marker of osteoarthritis [7]. A high profile editorial published in the British Medical Journal in January 2015 has fuelled the debate further. Lohmander and Roos highlighted the limited evidence for the need to reconstruct the ACL [8]. These authors used results from their own trial’s report published in 2010 to substantiate their claims [9]. In this randomized controlled trial it is suggested that structured rehabilitation may also be appropriate for younger active patients. In contrast, it is reported that over a third of patients who defer ACL reconstruction return for surgery within two years, deferred surgery was also associated with a higher incidence of meniscal injury requiring surgery [10-12]. The latter findings were robustly echoed in a large observational study of over 5000 patients with ACL rupture [12]. The presence of such contrasting opinions exhorts the need to investigate a balanced argument based on methodological appraisal of the best available evidence as well as considering other sources of evidence. Numerous trials only report a proportion of their principal outcome measures; this can lead to misinterpretation of evidence and creates a high risk of bias. Selective reporting can further distort the evidence base leading to the misrepresentation of advantages of interventions [13-21]. Makhni et al carried out a quantitative evaluation of variability in studies investigating ACLR. They analysed 119 studies published across all high impact factor orthopaedic literature. The authors found a high degree of variability in outcome reporting, with only 50% reporting objective outcome measures, and only 24% reporting return to pre-injury level of function. The authors noted also a high variability in instrumented assessment of laxity [22]. Consequently, a systematic review with meta-narrative analyses of studies, which compared ACL reconstruction vs. non-operative treatment with long-term results, was conducted in order to evaluate the literature and help formulate a baseline argument on the role of NLR as a possible source of evidence.
Methods
A systematic search of the literature was performed using terms related to: anterior cruciate ligament, reconstruction, surgical, operative, treatment, non-operative, non-surgical, immobilisation, physiotherapy, rehabilitation, brace. The search syntax, alternative keywords, and term variations were used across all database records. Search database utilised were: MEDLINE®, Embaseᵀᴹ, CINAHL® (cumulative index to nursing and allied health literature) and the Cochrane Central Register of Controlled Trials (CENTRAL) (Figure 1). Selected studies were used to evaluate quality and completion of main outcome measures reported in the ACL literature (summarised in tables 1 and 2).
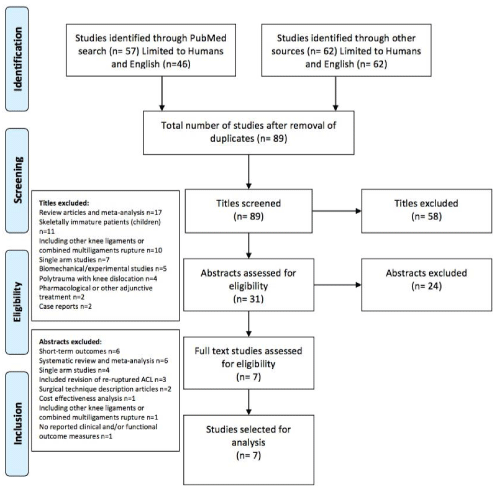
Figure 1: Flow diagram of studies selection process.
| Table 1: Summary of study parameters. | |||||||||
| Study | Numbers operative vs. non-op | Mean Age | Gender (M/F) | Injury to intervention Time (months) |
Diagnostic modality | Associated injury | Operative Treatment |
Non-Operative Treatment |
Follow up Mean & Range (years) |
| Fink et al.{Fink, 2001, Long-term outcome of operative or nonoperative treatment of anterior cruciate ligament rupture--is sports activity a determining variable?} | 113 (72 vs. 41) | Op: 36.6 Non-op 32.3 |
55/16 | 3.3 | Arthroscopy | 48% meniscal 15% MCL |
Open BPTB | Hamstring, cycling, swimming | 5-7 then 10-13 |
| Frobell et al. | 121 (62/59) | 26 | 88/32 | > 4 weeks? | MRI | 51% meniscal 31% chondral |
Arthroscopic BPTB or Hamstring | ? | 5 |
| Kessler et al. | 109 (60/49) | 30.7 | 68/41 | ? | Arthroscopy | 35% meniscal/ Chondral |
Arthroscopic BPTB | Brace 6/52 then gradual physio | 11.1 |
| Meuffels et al. | 50 (25/25) | Op 37.6 Non-op 37.8 |
38/12 | 6 (2-258) | Arthroscopy or MRI | 74% meniscal 38% chondral |
Open BPTB | Active rehab and ROM | 10 |
| Mihelic et al. | 54 (36/18) | Op 25.3 Non-op 25.5 |
44/10 | 19 | Arthroscopy | 28% MM 5% both menisci |
Open BPTB | POP 3 weeks. ROM & strength | 17-20 |
| Streich et al. | 80 (40/40) | Op: 26 Non-op: 24 |
56/24 | Op 7.3 Non-op 5.8 |
Arthroscopy | 24% partial meniscetomy | Arthroscopic BPTB | Close kinetic chain exercises | 15 |
| Swirtun et al. | 57 (22/35) | 32 | 30/27 | 9 | Arthroscopy or MRI | 37% meniscal or chondral | Arthroscopic BPTB | ? | 5.6 (5-6) |
| ?: Not reported. BPTB: bone patellar tendon bone. MRI: magnetic resonance imaging. MM: medial meniscus. MCL: medial collateral ligament. | |||||||||
| Table 2: Summary table for methodological evaluation of each study. | ||||||||||||
| Study | Design | Clearly outlined selection criteria | Random subject allocation | Allocation concealment | Baseline similarities of prognostic factors | Participants blinding | Blinding of intervention providers | Blinding of assessors of principal outcome measures | Minimum 85% complete follow-up with at least one principal outcome measure | Participants received allocated intervention or analysis by “intention to treat” | Reported comparison between groups for at least one principal outcome measure | Analysis of crude outcomes, variability and/or effect size |
| Fink et al. | Case series | Y | N | N | Y | N | N | N | Y | Y | Y | Y |
| Frobell et al. | RCT | Y | Y | N | Y | N | N | N | Y | Y | Y | Y |
| Kessler et al. | Case series | N | N | N | N | N | N | N | Y | Y | Y | Y |
| Meuffels et al. | Matched Therapeutic Series |
Y | N | N | Y | N | N | Y | Y | Y | Y | Y |
| Mihelic et al. | Case series | Y | N | N | N | N | N | N | Y | Y | Y | Y |
| Streich et al. | Case series | Y | N | N | Y | N | N | N | Y | Y | Y | Y |
| Swirtun et al. | Case series | Y | N | N | Y | N | N | N | Y | Y | Y | Y |
Results
Search results
A total of 119 records were generated from the search, limited to 108 humans and English publications. This yielded 89 titles for initial screening after removal of 19 duplicates. Following initial screening and application of the inclusion and exclusion criteria 58 titles and 24 abstracts were excluded. A further search including the cited references did not yield additional studies. The numbers and reasons for exclusion following rigorous titles screening, abstracts assessment and review of full texts are detailed in a flow diagram (Figure 1). Full-text review of the final studies was conducted. The final inclusion was therefore, a total of seven studies addressing the question and suitable for analysis.
Study characteristics
A summary of the study parameters is outlined in table 1. The seven studies analysed included a total of 584 patients, 317 were treated with ACL reconstruction and 267 received a non-operative management approach. The mean age of participants included was 30 years. Three of the studies reported combined ages for both interventions groups. The studies comprised 379 males and 162 females. At the exception of the RCT conducted by Frobell et al, all patients regardless of the intervention strategy received a diagnostic arthroscopy to confirm the status of ruptured ACL. The implication of this practice in terms of diagnostic accuracy and therapeutic effect is discussed below. Nevertheless, this practice is largely superseded nowadays by the wide availability of MRI scanning. Although three studies recorded the use of diagnostic MRI scanning, their overall utilisation was not adequately reported [23-25]. The mean interval between injury and treatment was 7.6 months, however this was inadequately recorded in two of the studies [23,26]. In addition, the duration prior to treatment was significantly variable from one to over 35 months [24,24]. The surgical intervention across all studies consisted of bone-patellar tendon-bone (BPTB) graft reconstruction. Frobell et al included patients who also received Hamstring grafts [23]. The non-operative management strategy consisted of exercise rehabilitation program followed by a gradual return to normal function including sports. Two studies adhered to an initial period of brace or splint immbolisiation [26,28]. All studies reported at least one principal outcome measure at a minimum of five years follow-up. The longest period of follow up was 20 years [28].
Methodological appraisal of studies
The study conducted by Frobell et al. was the only article, which compared the results of operative versus non-operative treatment using a randomised, controlled trial design [23]. The remaining six studies followed retrospective paired and non-paired comparisons. All studies achieved adequate follow up of results outlined in their outset. There was evidence of collection of at least one principal outcome measure in at least 85% of participants across all studies. In addition, five studies demonstrated baseline equivalence of potential prognostic factors between the two intervention groups. All seven studies reported comparison between groups for at least one principal outcome measure. A summary of the methodological evaluation for each study is presented in table 2. The results indicate that the current evidence-base portrays methodological limitations associated with a high risk of bias. With the exception of the RCT by Frobell et al. the remainder of the studies followed a subjective selection of participants determined by surgeon and/or patient’s choices. Given the designs of the studies there was no scope for blinding of assessors of intervention outcomes. Although it constituted a substantial source of bias, lack of blinding is a widely recognised design limitation in orthopaedic research [29,30]. Appraisal of the studies identified using a systematic approach revealed recurrent limitations and a high risk of bias. These observations are echoed in previous studies [1,31]. Consequently, the ability to determine the true extent of differences between the two interventions was significantly mitigated.
The meta-narrative results were analysed according to the key areas representing the most important study parameters, prognostic factors and outcome measures. These domains should constitute the focus of attention for completeness of outcome measures comparing ACLR and non-operative interventions. Following analysis of the key concepts it was possible to establish the relationships between the studies as well as identify areas where incomplete and variable outcome measures had occurred. The numbers of surgeons involved were not fully disclosed in three [23,24,27], out of the seven studies, and two of the studies used age as selection criteria for ACLR [23,27], while the remainder relied on subjective criteria depending on surgeons and patients preferences. In addition, five studies relied solely on arthroscopy for diagnosis, indicating that patients who did not receive ACLR still had a surgical intervention [23,26-28,32]. Similarly, four studies reported the use of open surgical technique [24,27,28,32], one study used both open and arthroscopic with no report of subset analysis in relation to technique or graft choice [26]. The average interval between diagnosis and surgical intervention varied greatly with a mean lead-time between three and nine months. Postoperative immobilisation was also variable, one study did not report on this important aspect of management [25,28], the remainder of studies ranged from two to six weeks in cast or knee brace. None of the studies defined the pattern of meniscal injury and meniscal status following initial treatment. Furthermore, three studies did not report the proportion of injured knee associated with meniscal lesions [25,28]. When reported, the incidence varied markedly between 23% and 80%. The proportion of meniscal lesion requiring operative treatment was not clearly reported in four out of the seven studies [24,25,28,32]. Nevertheless, the remaining studies indicated an increased risk of secondary meniscal surgery following non-operative management of two to four folds when compared to patients treated with ACLR. While graft rupture was the most commonly reported complication, five studies did not report adverse events following each intervention [23-27]. ACLR revision surgery was only reported in three of the studies [26,27]. Among these Kessler et al excluded this group from their final analysis [26]. In terms of knee stability evaluation, none of the studies used evaluation of knee stability in pre-operative assessment or as part of patient’s selection. KT 1000 and post-operative Lachman test were reported in five studies, demonstrating better results in ACLR groups. Streich et al showed no difference in KT 1000, [32], and Frobell et al demonstrated improved results in Lachman and Pivot Shift tests [23], results were not however clearly outlined for the subgroup treated with physical rehabilitation alone. Swirtun et al used neither clinical nor objective measurement of knee stability [25].
Discussion
ACL registries as an alternative source of evidence, lessons learned
In a report from the Swedish national ligament registry [33], 95% of primary ACL reconstruction was carried out using hamstring auto-graft in 2012. This was an increase from 80% in 2005. The registry showed that an entire primary ACL reconstruction population had a rate of 33% meniscal injuries and 27% chondral injuries [33,34]. When compared to BPTB the revision rates were similar, however patients who had undergone hamstring reconstruction demonstrated better functional scores at 5 years post-operatively. The cumulative risk of revision following primary ACLR was 3.3% and this increased to 5.7% in patients younger than 19 years. In the same report, female patients scored worse than male counterparts for return to sports and pre-injury level of activity, corroborating previous biomechanical studies, which suggested that female athletes have a more ligament dominated knee stability [33].
In the US, The Multicenter Orthopaedic Outcomes Network (MOON) consortium was created in 2002 to enroll and longitudinally follow a large population cohort of ACLR [35]. Although only limited to seven large centres it has been reported that the MOON cohort has had an important influence on the management of ACL rupture. The MOON collected database led to changes in ACLR practice including the use of auto-graft for high school, college, and competitive athletes in their primary anterior cruciate ligament reconstructions [35]. Other modifications included treatment options for meniscus and cartilage injuries, as well as lifestyle choices made after anterior cruciate ligament reconstruction [35]. The same long-term results have also helped the evaluation of societal and economic impact of ACL ruptures [4], ACLR was shown to be more cost effective compared to rehabilitation alone when taking into consideration indirect costs such as work and earnings [4,36]. In addition, the California (US) based Kaiser-Permante ACL cohort clearly defined patients related factors in the indication for early ACL reconstruction, based on initial knee stability testing and pre-injury levels of sports participation [37]. The rate of late primary reconstruction was 16% compared to the 51% recorded in the RCT by Frobell et al. [23,37]. The same database showed no correlation between severity of initial injury and late onset degenerative changes, suggesting a greater link to knee stability and level of functional demand [37,38]. Similar results were echoed in the Delaware-Oslo ACL cohort akin to a multicenter clinical registry. The latter group also demonstrated the importance of patients and activity level on long-term outcomes at 10 years following ACL injury. They demonstrated that a subset of patients could be managed with rehabilitation alone [39,40]. The severity of initial knee instability, activity level and functional demand measured on KOOS score were outlined as useful cutoff variance for patients potentially able to derive good outcomes from non-operative treatment [40]. The reported incidence of associated meniscal injuries in the earlier literature varied markedly between 23% and 80% [23-28]. UK-NLR demonstrated comparable figures to previous observational studies [12,41,42].
Results from the MOON cohort enabled the creation a vast plethora of evidence on patients’ risk factors and ACL reconstruction outcomes, rate of graft failures, and outcomes in relation to concomitant soft tissue knee injuries [43]. In contrast, information about surgical outcome and adverse events following ACLR in the UK had been traditionally confined to limited series from individual surgeons and specialized units [44].
Another useful role for the registry is the ability to use cumulative revision rates of primary ACLR and correlate these with the various prognostic factors stipulated in earlier studies. For instance a recent study derived from the Kaiser Permante ACL registry (California, USA) has demonstrated that femoral drilling technique and graft fixation devices had markedly changed over the last seven years, even though cumulative ACLR revision rates remained stable [45].
Why do we need a UK ACL registry?
Traditionally, studies influencing technical choices included biomechanical in-vitro analyses, as well as successes and failures reported in experimental studies or case series. In comparison the ACL registry will include prospective data collection from all centres hence reducing the risk of recall and selection bias. Consequently, even surgeons from low volume institutions will become able to compare and if needed alter their practice in order to improve outcomes. Furthermore, recommendation on timing of intervention, need for associated procedures, and surgical volumes can be derived from such registries. Even though lessons can be learned from other ACL registries, the need for a UK based ACL registry had become vital. There are variations in the patients’ populations and local practices across the already established registries. This has been outlined in the reported differences in techniques and outcomes from The Danish knee ligament registry and the MOON group [46,47]. Therefore, our own national registry will not only help influence local practice and research but also allow comparison with other registries at an international level.
Potential shortfalls
At present clinical registries globally suffer from unattained full potential. The latter often stems from limitations in the validity and accuracy of data collected. A recent study comparing NJR data with the London Implant Retrieval Centre reported that 39.1% of retrieved implants were not recorded by the NJR [48]. Similarly, in other registries such as the Scandinavian hip registry only 67% of prosthetic infection were accurately recorded when compared to other sources, namely prescription registries, lab results and disease surveillance studies [49]. This global situation is not limited to clinical data. Another recent study identified discrepancies in demographic as well as comorbidities information when comparing trauma registries in the US [50].
In addition, the registry in its original version relied on patients’ access to the Internet and a valid email address. Access to an email address, computer literacy, and loss of email contact due to spam filter or fear of Internet fraud might be at the source of this limiting factor [51,52].
Conclusion and Future Solutions
The ability to evaluate a large number of patients in various settings and to evaluate multiple exposures and outcomes simultaneously offers a clear advantage as an additional source of evidence base. The focus of future work should be on registry data evaluation and data quality assurance, drawing lessons from the benchmark established by the NJR. The future for UK-NLR data quality assurance will be to replicate the practice established by the NJR especially the NJR data quality audit. The latter has been rolled-out on a national program of local data completeness and accuracy audits, following the development of an audit toolkit during a six hospitals pilot phase [53]. The majority of NHS trusts have participated using a standardised approach to facilitate and support the audit process. A data migration process, a so called “push to registry” function, using available technologies can also help harmonise data collection without the additional load on clinical teams. Linking the registry to clinical databases can be laborious and financially demanding. However, this approach is technically achievable and has gained international acceptance as illustrated by models from arthroplasty registries.
REFERENCES
- Linko E, Harilainen A, Malmivaara A, Seitsalo S. Surgical versus conservative interventions for anterior cruciate ligament ruptures in adults. Cochrane Database Syst Rev. 2005. Ref.: https://goo.gl/fwqQD6
- Kwok CS, Harrison T, Servant C. The optimal timing for anterior cruciate ligament reconstruction with respect to the risk of postoperative stiffness. Arthroscopy. 2013; 29: 556-565. Ref.: https://goo.gl/p3Hzfk
- Smith TO, Davies L, Hing CB. Early versus delayed surgery for anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc. 2010; 18: 304-311. Ref.: https://goo.gl/rJMNKN
- Mather RC 3rd, Koenig L, Kocher MS, Dall TM, Gallo P, et al. Societal and economic impact of anterior cruciate ligament tears. J Bone Joint Surg Am. 2013; 95: 1751-1759. Ref.: https://goo.gl/k25ZnU
- Chalmers PN, Mall NA, Moric M, Sherman SL, Paletta GP, et al. Does ACL reconstruction alter natural history?: A systematic literature review of long-term outcomes. J Bone Joint Surg Am. 2014; 96: 292-300. Ref.: https://goo.gl/1DSZpt
- Kapoor B, Clement DJ, Kirkley A, Maffulli N. Current practice in the management of anterior cruciate ligament injuries in the United Kingdom. Br J Sports Med. 2004; 38: 542-544. Ref.: https://goo.gl/r9mJnu
- Nordenvall R, Bahmanyar S, Adami J, Mattila VM, Felländer-Tsai L. Cruciate ligament reconstruction and risk of knee osteoarthritis: the association between cruciate ligament injury and post-traumatic osteoarthritis. a population based nationwide study in Sweden, 1987-2009. PLoS One. 2014; 9. Ref.: https://goo.gl/HazmXG
- Lohmander LS, Roos EM. The evidence base for orthopaedics and sports medicine. Bmj. 2015; 350. Ref.: https://goo.gl/yHSzek
- Frobell RB, Roos EM, Roos HP, Ranstam J, Lohmander LS. A randomized trial of treatment for acute anterior cruciate ligament tears. N Engl J Med. 2010; 363: 331-342. Ref.: https://goo.gl/pFrWgW
- Levy BA. Is early reconstruction necessary for all anterior cruciate ligament tears? N Engl J Med. 2010; 363: 386-388. Ref.: https://goo.gl/H51jXb
- Richmond JC, Lubowitz JH, Poehling GG. Prompt operative intervention reduces long-term osteoarthritis after knee anterior cruciate ligament tear. Arthroscopy. 2011: 27: 149-52. Ref.: https://goo.gl/XSBfDP
- Sri-Ram K, Salmon LJ, Pinczewski LA, Roe JP. The incidence of secondary pathology after anterior cruciate ligament rupture in 5086 patients requiring ligament reconstruction. Bone Joint J. 2013; 95: 59-64. Ref.: https://goo.gl/fCDPBf
- Dwan K, Gamble C, Williamson PR, Kirkham JJ, Reporting Bias Group. Systematic review of the empirical evidence of study publication bias and outcome reporting bias - an updated review. PLoS One. 2013; 8. Ref.: https://goo.gl/GWyCbr
- Chan AW, Song F, Vickers A, Jefferson T, Dickersin K, et al. Increasing value and reducing waste: addressing inaccessible research. Lancet. 2014; 383: 257-266. Ref.: https://goo.gl/vFjpZ5
- Chan AW, Krleza-Jeric K, Schmid I, Altman DG. Outcome reporting bias in randomized trials funded by the Canadian Institutes of Health Research. Cmaj. 2004; 171: 735-740. Ref.: https://goo.gl/eg5JuL
- Shamliyan T, Kane RL. Clinical research involving children: registration, completeness, and publication. Pediatrics. 2012; 129. Ref.: https://goo.gl/M3wRqn
- Bourgeois FT, Murthy S, Mandl KD. Outcome reporting among drug trials registered in ClinicalTrials.gov. Ann Intern Med. 2010; 153: 158-166. Ref.: https://goo.gl/NtXx3X
- Turner EH, Matthews AM, Linardatos E, Tell RA, Rosenthal R. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med. 2008; 358: 252-260. Ref.: https://goo.gl/5DcFXT
- Chalmers I. Underreporting research is scientific misconduct. Jama. 1990; 263: 1405-1408. Ref.: https://goo.gl/9c1q2c
- Smyth RM, Kirkham JJ, Jacoby A, Altman DG, Gamble C, et al. Frequency and reasons for outcome reporting bias in clinical trials: interviews with trialists. Bmj. 2011; 342. Ref.: https://goo.gl/fypysz
- Saini P, Loke YK, Gamble C, Altman DG, Williamson PR, et al. Selective reporting bias of harm outcomes within studies: findings from a cohort of systematic reviews. Bmj. 2014; 349. Ref.: https://goo.gl/38qTuY
- Makhni EC, Padaki AS, Petridis PD, Steinhaus ME, Ahmad CS, et al. High Variability in Outcome Reporting Patterns in High-Impact ACL Literature. J Bone Joint Surg Am. 2015; 97: 1529-1542. Ref.: https://goo.gl/1hy5ka
- Frobell RB, Roos HP, Roos EM, Roemer FW, Ranstam J, et al. Treatment for acute anterior cruciate ligament tear: five year outcome of randomised trial. Bmj. 2013; 346. Ref.: https://goo.gl/qxC93j
- Meuffels DE, Favejee MM, Vissers MM, Heijboer MP, Reijman M, et al. Ten year follow-up study comparing conservative versus operative treatment of anterior cruciate ligament ruptures. A matched-pair analysis of high level athletes. Br J Sports Med. 2009; 43: 347-351. Ref.: https://goo.gl/T82rB5
- Swirtun LR, Renstrom P. Factors affecting outcome after anterior cruciate ligament injury: a prospective study with a six-year follow-up. Scand J Med Sci Sports. 2008; 18: 318-324. Ref.: https://goo.gl/zZgNQV
- Kessler MA, Behrend H, Henz S, Stutz G, Rukavina A, et al. Function, osteoarthritis and activity after ACL-rupture: 11 years follow-up results of conservative versus reconstructive treatment. Knee Surg Sports Traumatol Arthrosc. 2008; 16: 442-448. Ref.: https://goo.gl/ycJ2H8
- Fink C, Hoser C, Hackl W, Navarro RA, Benedetto KP. Long-term outcome of operative or nonoperative treatment of anterior cruciate ligament rupture--is sports activity a determining variable? Int J Sports Med. 2001; 22: 304-309. Ref.: https://goo.gl/FEJPX8
- Mihelic R, Jurdana H, Jotanovic Z, Madjarevic T, Tudor A. Long-term results of anterior cruciate ligament reconstruction: A comparison with non-operative treatment with a follow-up of 17-20 years. International Orthopaedics. 2011; 35: 1093-1097. Ref.: https://goo.gl/2ciqy8
- Poolman RW, Struijs PA, Krips R, Sierevelt IN, Marti RK, et al. Reporting of outcomes in orthopaedic randomized trials: does blinding of outcome assessors matter? J Bone Joint Surg Am. 2007; 89: 550-558. Ref.: https://goo.gl/9QQ8hr
- Hrobjartsson A, Thomsen AS, Emanuelsson F, Tendal B, Rasmussen JV, et al. Observer bias in randomized clinical trials with time-to-event outcomes: systematic review of trials with both blinded and non-blinded outcome assessors. Int J Epidemiol. 2014; 43: 937-948. Ref.: https://goo.gl/EMMto8
- Smith TO, Postle K, Penny F, McNamara I, Mann CJ. Is reconstruction the best management strategy for anterior cruciate ligament rupture? A systematic review and meta-analysis comparing anterior cruciate ligament reconstruction versus non-operative treatment. Knee. 2014; 21: 462-470. Ref.: https://goo.gl/LD7vEQ
- Streich NA, Zimmermann D, Bode G, Schmitt H. Reconstructive versus non-reconstructive treatment of anterior cruciate ligament insufficiency. A retrospective matched-pair long-term follow-up. Int Orthop. 2011; 35: 607-613. Ref.: https://goo.gl/YBGcy4
- Kvist J, Kartus J, Karlsson J, Forssblad M. Results from the Swedish national anterior cruciate ligament register. Arthroscopy. 2014; 30: 803-810. Ref.: https://goo.gl/1UcyMw
- Ahlden M, Samuelsson K, Sernert N, Forssblad M, Karlsson J, et al. The Swedish National Anterior Cruciate Ligament Register: a report on baseline variables and outcomes of surgery for almost 18,000 patients. Am J Sports Med. 2012; 40: 2230-2235. Ref.: https://goo.gl/1y1F4t
- Lynch TS, Parker RD, Patel RM, Andrish JT, MOON Group, et al. The Impact of the Multicenter Orthopaedic Outcomes Network (MOON) Research on Anterior Cruciate Ligament Reconstruction and Orthopaedic Practice. J Am Acad Orthop Surg. 2015; 23: 154-163. Ref.: https://goo.gl/72ZgNE
- Mather RC, 3rd, Hettrich CM, Dunn WR, Cole BJ, Bach BR Jr, et al. Cost-Effectiveness Analysis of Early Reconstruction Versus Rehabilitation and Delayed Reconstruction for Anterior Cruciate Ligament Tears. Am J Sports Med. 2014; 42: 1583-1591. Ref.: https://goo.gl/kWLd6y
- Fithian DC, Paxton EW, Stone ML, Luetzow WF, Csintalan RP, et al. Prospective trial of a treatment algorithm for the management of the anterior cruciate ligament-injured knee. Am J Sports Med. 2005; 33: 335-346. Ref.: https://goo.gl/cJpDHv
- Fithian DC. To Operate or Not to Operate? That Is (Still) the Question: Commentary on an article by Hege Grindem, PT, PhD, et al.: "Nonsurgical or Surgical Treatment of ACL Injuries: Knee Function, Sports Participation, and Knee Reinjury. The Delaware-Oslo ACL Cohort Study". J Bone Joint Surg Am. 2014; 96. Ref.: https://goo.gl/eTVCVi
- Grindem H, Eitzen I, Engebretsen L, Snyder-Mackler L, Risberg MA. Nonsurgical or Surgical Treatment of ACL Injuries: Knee Function, Sports Participation, and Knee Reinjury: The Delaware-Oslo ACL Cohort Study. J Bone Joint Surg Am. 2014; 96: 1233-1241. Ref.: https://goo.gl/Lkb7QP
- Hurd WJ, Axe MJ, Snyder-Mackler L. A 10-year prospective trial of a patient management algorithm and screening examination for highly active individuals with anterior cruciate ligament injury: Part 1, outcomes. Am J Sports Med. 2008; 36: 40-47. Ref.: https://goo.gl/6RyHXt
- Bray RC, Dandy DJ. Meniscal lesions and chronic anterior cruciate ligament deficiency. Meniscal tears occurring before and after reconstruction. J Bone Joint Surg Br. 1989; 71: 128-130. Ref.: https://goo.gl/aYQiEU
- Robb C, Kempshall P, Getgood A, Standell H, Sprowson A, et al. Meniscal integrity predicts laxity of anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2015; 23: 3683-3690. Ref.: https://goo.gl/KqehRu
- Fetzer GB, Spindler KP, Amendola A, Andrish JT, Bergfeld JA, et al. Potential market for new meniscus repair strategies: evaluation of the MOON cohort. J Knee Surg. 2009; 22: 180-186. Ref.: https://goo.gl/rERJNz
- Jameson SS, Dowen D, James P, Serrano-Pedraza I, Reed MR, et al. Complications following anterior cruciate ligament reconstruction in the English NHS. Knee. 2012; 19: 14-19. Ref.: https://goo.gl/unDQmb
- Tibor L, Chan PH, Funahashi TT, Wyatt R, Maletis GB, et al. Surgical Technique Trends in Primary ACL Reconstruction from 2007 to 2014. J Bone Joint Surg Am. 2016; 98: 1079-1089. Ref.: https://goo.gl/YEjsgx
- Duffee A, Magnussen RA, Pedroza AD, Flanigan DC, MOON Group, et al. Transtibial ACL femoral tunnel preparation increases odds of repeat ipsilateral knee surgery. J Bone Joint Surg Am. 2013; 95: 2035-2042. Ref.: https://goo.gl/XuVKN5
- Rahr-Wagner L, Thillemann TM, Pedersen AB, Lind M. Comparison of hamstring tendon and patellar tendon grafts in anterior cruciate ligament reconstruction in a nationwide population-based cohort study: results from the danish registry of knee ligament reconstruction. Am J Sports Med. 2014; 42: 278-284. Ref.: https://goo.gl/bUAVKD
- Sabah SA, Henckel J, Cook E, Whittaker R, Hothi H, et al. Validation of primary metal-on-metal hip arthroplasties on the National Joint Registry for England, Wales and Northern Ireland using data from the London Implant Retrieval Centre: a study using the NJR dataset. Bone Joint J. 2015; 97: 10-18. Ref.: https://goo.gl/NqNh97
- Gundtoft PH, Pedersen AB, Schonheyder HC, Overgaard S. Validation of the diagnosis 'prosthetic joint infection' in the Danish Hip Arthroplasty Register. Bone Joint J. 2016; 98: 320-325. Ref.: https://goo.gl/hfrD5S
- Samuel AM, Lukasiewicz AM, Webb ML, Bohl DD, Basques BA, et al. Do we really know our patient population in database research? A comparison of the femoral shaft fracture patient populations in three commonly used national databases. Bone Joint J. 2016; 98: 425-432. Ref.: https://goo.gl/VfnBvU
- Atherton H, Sawmynaden P, Sheikh A, Majeed A, Car J. Email for clinical communication between patients/caregivers and healthcare professionals. Cochrane Database Syst Rev. 2012; 11. Ref.: https://goo.gl/zN8pYT
- Haun JN, Patel NR, Lind JD, Antinori N. Large-Scale Survey Findings Inform Patients' Experiences in Using Secure Messaging to Engage in Patient-Provider Communication and Self-Care Management: A Quantitative Assessment. J Med Internet Res. 2015; 17. Ref.: https://goo.gl/yhH19w
- National Joint Registry: Supporting Data Quality. 2016.