Research Article
Use of Hand Rehabilitation Board (Dominic’s Board) in Post Traumatic/Stroke Rehabilitation of the Upper Limbs
Dominic Essien and Christopher Ekpenyong*
Department of Physiology, Faculty of Basic Medical Sciences, University of Uyo, Uyo, Nigeria
*Address for Correspondence: Dr. Christopher E. Ekpenyong, Department of Physiology, Faculty of Basic Medical Sciences, University of Uyo, Akwa Ibom State, Nigeria, Tel: +2348023347719; Email: [email protected]; [email protected]
Dates: Submitted: 14 April 2017; Approved: 29 May 2017; Published: 31 May 2017
How to cite this article: Dominic Essien, Christopher Ekpenyong. Use of Hand Rehabilitation Board (Dominic’s Board) in Post Traumatic/Stroke Rehabilitation of the Upper Limbs. J Sports Med Ther. 2017; 2: 057-065. DOI: 10.29328/journal.jsmt.1001009
Copyright License: © 2017 Essien D, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Dominic’s board; Hand; Injuries; Deformities: Rehabilitation

ABSTRACT
In recent years, the increasing number of patients with upper limb musculoskeletal disorders seeking timely, intensive, prolonged and task oriented hospital- and home- based physical rehabilitation, and the decreasing numbers of trained therapist to provide the needed care, have left a palpable gab. These have resulted in several preventable deformities with associated complications leading to social and economic burdens. Although the introduction of some robotic devices has addressed some of these concerns, the shortfalls from the use of these devices limit their effectiveness. The newly introduced hand rehabilitation board (Dominic’s Board) was prospectively evaluated in 82 patients with ULMDs of different etiologies to assess its therapeutic efficacy in rehabilitation of ULMDs. Additive, but complementary effect was observed when used along with conventional hospital-based therapy and at home, suggesting the effectiveness of this device in preventing or ameliorating the complications associated with ULMDs.
INTRODUCTION
Upper limb musculoskeletal disorders (ULMDs) are disorders affecting muscles, bones, tendons, nerves and blood vessels of the neck, shoulders, elbows, arms and hands [1]. They are common and debilitating and are associated with functional impairment including interference with daily activities such as eating, dressing, washing clothes, difficulty shopping and carrying a shopping bag as well as difficulty with hobbies. There are growing numbers of patients with ULMDs leading to varying prevalence across different populations. However, the prevalence ranges from 58% to 81% [2,3] and may be influenced by the socio-demographic characteristics of the study participants and other covariates. Due to the high prevalence and associated disabilities, ULMDs frequently lead to higher health care use with many patients presenting in the primary care centers and rheumatology clinics [4]. Because these deformities limit patients’ upper limb functionality, and hence independence, they are always in dire need for assistant both at the rehabilitation centers and at home. Also, since the restoration of upper limb functionality depends significantly on the onset, duration, intensity and task orientation of the training [5], home based physical therapy/care has become a significant component of physical rehabilitation of patients with ULMDs. However, the increasing demand for home base physical therapy/care is despite the unavailability of enough trained therapist and care givers to provide this very important component of rehabilitation therapy and care. Trained physiotherapists are few, and are hardly available for effective rehabilitation of the patients following injuries of any kind. Their scarcity makes it difficult to give enough time for the rehabilitation of patients with these deformities.
Accordingly, [3,5] acknowledged that the existing shortage of trained therapist and caregivers for home-based care is expected to increase and become serious problem. Given the lack of man power to effect prompt, prolonged, intense and effective physical rehabilitation at health facilities and the associated boredom that accompanies repetitive movement especially on the part of the therapist, it becomes a great necessity to produce devices that can help patients to perform these repetitive movements unassisted especially at home, and when in isolation. These devices can help provide continuous and intense physical rehabilitation at home since hospital based rehabilitation time is getting shorter and shorter due to economic reasons Maciejasz who cited Richards et al. [6].
The hand rehabilitation board is a novel piece of device that allows the patient to independently carry out repetitive exercises over many hours, days and for a long period of time. This device makes it possible for patients to move the upper limb in all directions at home without supervision and/ or assistance. Evidence has however shown that a greater dose of an intervention is better than a lesser dose of intervention [2]. Although several devices have been used attempting to achieve similar purpose, only few of them have actually reached the targeted population [5]. Also, the outcome of those already in use is not as positive as expected Maciejasz who cited Patton et al. [7], due to several associated shortfalls from their uses.
Furthermore, their availability is greatly limited in developing countries and in particular poor communities with limited access to and usage of health facilities and where a great number of these patients reside [3]. Given these, there is still a significant need to improve efficiency and reduce cost of home-based devices for therapy [5]. It was in the light of this that the hand rehabilitation board was conceived in an attempt to bridge the gap between the scarcities of trained physiotherapist, short falls from the use of some robotic devices and the multitude of patients who earnestly need physical rehabilitation especially the upper limb rehabilitation. Often patients who are dissatisfied with their current treatments will discontinue shortly after and seek alternative/complementary treatments [5].
MATERIAL AND METHODS
Selection and grouping of subjects
This study was conducted in a physical rehabilitation center in Uyo metropolis, Southern Nigeria between the months of March and October 2016, Eighty-two patients (48 males and 34 females) with various forms of upper limb injuries/disorders were prospectively studied to assess the therapeutic efficacy of Dominic’s physical rehabilitation board in restoring their upper limb functionality. They were selected from patients with ULMDs who had their conventional treatments including immobilization for at least two weeks, and also stroke patients with stable blood pressure. These patients were subdivided into 3 groups; those undergoing conventional treatment (soft tissue manipulation, finger steps, proprioceptive neuro-muscular facilitation, infrared radiation therapy, and exercise) (group1), those on conventional treatment who also used Dominic’s physical rehabilitation board for at least one hour or as they can tolerate during visit to the rehabilitation center (group 2), and those who were on conventional treatment plus use of Dominic’s Board on visiting the rehabilitation center and at home (group 3). The treatment lasted for three months. The socio-demographic characteristics of the study participants were assessed using standard instruments.
MATERIALS
Instruments of measurement
• Dominic’s Physical Rehabilitation Board
• Goniometer for measuring angle of extension of joints. The Goniometric measurement was done before the commencement of the study and at the end of three months.
• A semi-structured, self-administered questionnaire on socio-demographic characteristics of participants and causes of ULMDS.
METHODS
• The wooden square comfortably kept on a normal height table.
• The four poles are fixed on each of the four wooden blocks and locked into positions.
• The eighteen circular wooden plates are stacked on one of the four wooden poles.
• With the device ready for use, a comfortable chair with back support is kept by the table on which the patient sits and commences the exercise.
Mechanism of action
The movement of the wooden plates from one pole into the other and round the four poles on the square wooden plate brings about all the desired movements in the upper limb. The square wooden plate is placed such that the poles are oriented right (a), left (b), distally (c) and proximally (d).
Assessment measures
The efficacy of Dominic’s physical rehabilitation board was evaluated on 82 patients with various forms of ULMDs, after obtaining duly informed consent. For each of the 3 groups of patients, the hand functionality and mobility were assessed before and after the use of the rehabilitation board. However, patients in all groups were administered the same conventional treatment (e.g., infrared radiation and chemotherapy).
STATISTICAL ANALYSIS
Data obtained were analyzed using frequencies, percentages, means, standard error of mean (SEM), paired t-test, analysis of variance (ANOVA) (one-way) followed by Duncan’s test. Frequencies and percentages were used to analyze demographic characteristics of the participants and distribution of the causes of deformity among the subjects. The magnitudes of arm extension between groups were computed and results were expressed as mean ± SEM.
Significant differences in the degree of arm extension were tested using one-way ANOVA followed by Duncan’s test. Statistical significance was established at 5% (p<0.05). Data were analyzed using the Statistical Package for Social Science version 20.0 (SPSS). Furthermore, differences in magnitude of arm extension before and after treatment with Dominic’s Board, in relation to groups and causes of deformity was assessed using paired t-test.
RESULTS
The socio-demographic characteristics of the study subjects showed that a greater number of them were males (58.5%) with ages between 31 and 40 years (35.3%), employed (63.4%), physically active (75.6%), single (59.8%) and with secondary school level of education (46.3%) (Table 1).
| Table 1: socio-demographic characteristics of study participants. | |
| Variables | Number (%) |
| Sex Male Female |
48 (58.5) 34 (14.5) |
| Age < 18 18-30 31-40 41-50 >50 |
14 (17) 16 (19.5) 29 (35.3) 11 (13.4) 12 (14.6) |
| Employment status Employed Unemployed |
52 (63.4) 30 (36.6) |
| Physical activity status Active Inactive |
62 (75.6) 20 (24.4) |
| Marital status Single Married |
49 (59.85) 33 (40.2) |
| Educational qualification Primary education Secondary Tertiary |
26 (31.7) 35 (46.3) 18 (22.0) |
Table 2 shows the common causes of ULMDs, frequency of ULMDs and the recovery rate after conventional treatment and rehabilitation with Dominic’s physical rehabilitation board at physical rehabilitation center and at home. The major causes of ULMDs in descending order are road traffic accident (23 subjects), industrial accident (17 subjects), stroke (12 subjects), sport injuries (10 subjects), arthritis (8 subjects) traumatic injuries other than RTA (6 subjects), and cerebral palsy (5 subjects). The highest rate of recovery was achieved by participants with ULMDs due to unknown etiology (100%), followed by sport injuries (90%), traumatic injuries other than RTA (83.3%), stroke (83%), cerebral palsy (80%), RTA (78.3%), arthritis (75%), and industrial accident (70.6%).
| Table 2: causes and frequencies of ULMDs. | |||
| S/N | Causes of deformity | Frequency | Recovery rates |
| 1 | Road traffic accident (RTA) | 23 | 18 (78.3%) |
| 2 | Sport injury | 10 | 9 (90%) |
| 3 | Traumatic injuries other than RTA | 6 | 5 (83.3%) |
| 4 | Industrial accident | 17 | 12 (70.6%) |
| 5 | Cerebral palsy | 5 | 4 (80%) |
| 6 | Osteoarthritis | 8 | 6 (75%) |
| 7 | Cerebrovascular accident (stroke) | 12 | 10 (83.3%) |
| 8 | Idiopathic | 1 | 1 (100%) |
Participants in group 3 who were managed with conventional therapy and Dominic’s physical rehabilitation board at the physical rehabilitation center and at home achieved the highest degree of arm mobility and functionality than those in groups 1 and 2. In a similar manner, those in group 2 achieved a higher degree of arm mobility and functionality than those in group 1 (Table 3 and 4, and figure 1).
| Table 3: extension of the arm between groups in relation to causes of ULMDs. | ||||
| Treatment Groups | Cause of upper limb musculoskeletal disorders | Before treatment with Dominic’s Board | After treatment with Dominic’s Board | P-value |
| Conventional treatment only(G1) | Stroke | 28.71 ± 8.87 | 54.14 ± 12.38 | 0.002 |
| Traumatic injury | 14.17 ± 3.19 | 86.00 ± 15.04 | 0.002 | |
| Conventional treatment and Dominic’s Board at the cener only(G2) | Stroke | 19.33 ± 5.90 | 96.83 ± 15.69 | 0.001 |
| Traumatic injury | 11.33 ± 1.41 | 114.67 ± 7.26 | 0.000 | |
| Conventional treatment and Dominic’s Board at the center& at home(G3) | Traumatic and Stroke related injuries |
30.67 ± 12.16 | 156.67 ± 13.98 | 0.000 |
| Table 4: gain in arm extension between groups. | |
| Groups | Mean ± SEM |
| 1 | 46.85 ± 8.86a |
| 2 | 90.42 ± 7.13b |
| 3 | 26.00 ± 11.70c |
| Different superscript means significantly different at 5% (p<0.05) | |
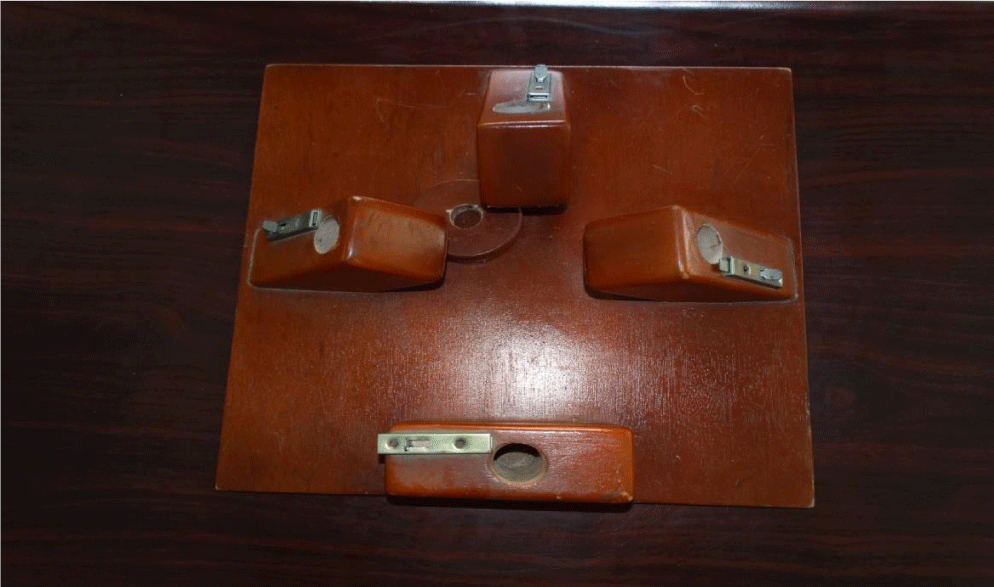
Figure 1: A Child with left Shoulder injury using Dominic’s Physical Rehabilitation Board during her rehabilitation phase.
DISCUSSION
Findings of the present study suggest the effectiveness of Dominic’s physical rehabilitation board in restoring upper limb functionality in patients with ULMDs regardless of the etiology. The results further confirmed the hypothesis that a higher dose of an intervention (measured by duration and frequency) is therapeutically more effective than a lower dose of an intervention.
Accordingly, participants who received conventional treatments and also used Dominic’s physical rehabilitation board at the physical therapy center and at home (group 3) recorded the highest recovery rate of upper limb functionality (measured by ability to wash the hand, bath one’s self, eat independently, write, wash simple clothing, flip affected fingers, drink, dress one’s self, pronate and supinate the affected hand). Also, improvements in multidirectional upper limb mobility (measured by angle of extension, flexion, pronation, supination, abduction and adduction) were more in participants in group 3 than 2, and better in group 2 than group 1.
The special features/components of Dominic’s physical rehabilitation board such as the four wooden blocks with poles, eighteen pieces of circular wooden plates are accurately positioned to enhance virtually all forms of movements of the upper limb including extension, flexion, abduction, adduction, pronation supination and retraction. Interestingly, these movements occur in virtually all the joints of the upper limb (shoulder, elbow, wrist, phalangeal and interphalangeal joints) and in all directions as shown the figures 2 to 13. By moving the circular wooden plates from one pole to the other and round the four poles on the square wooden plate, all the above mentioned desired movements of the upper limb are achieved. These circular wooden plates are placed such that the poles are oriented left, right, proximally and distally.

Figure 2: A square board measuring 16 by16 inches in length and width with 4 wooden blocks placed on each of the four sides. Each of the four wooden blocks has a hole in the upper one third that bears a wooden pole. Each of the wooden blocks is inclined at 600 to the floor of the wooden square.

Figure 3: Four wooden poles, each having a length of 18 inches and a base of 3 inches that normally fit into the hole on the wooden block.

Figure 4: Eighteen pieces of circular wooden plates, ranging from 1.5 inches to 7.0 inches in diameter with a thickness of 0.5 inch.

Figure 5: In a sitting position, the left upper limb moves into adduction by moving the wooden circular plates to the right pole (a).

Figure 6: The left upper limb moves into abduction by moving the wooden circular plates to the left wooden pole (b).

Figure 7: The right upper limb moves into extension by moving the wooden circular plates to the distal wooden pole (c).
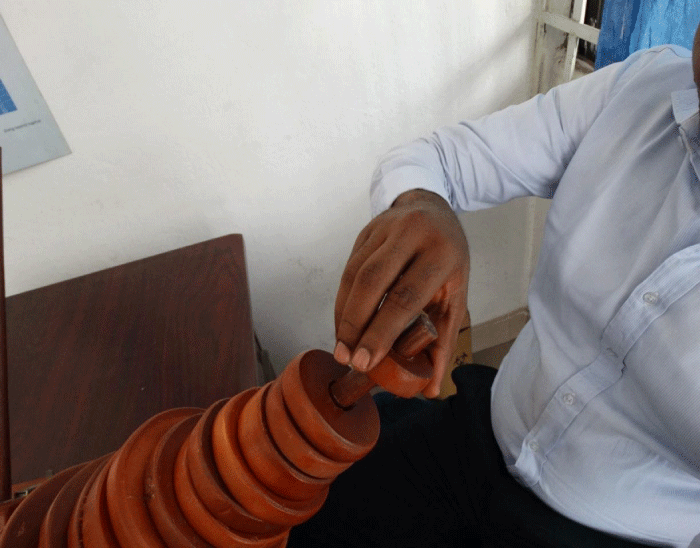
Figure 8: The right upper limb moves into retraction as well as elbow flexion by moving the wooden circular plates to the proximal pole (d).

Figure 9: The inter-phalangeal joints go into flexion..
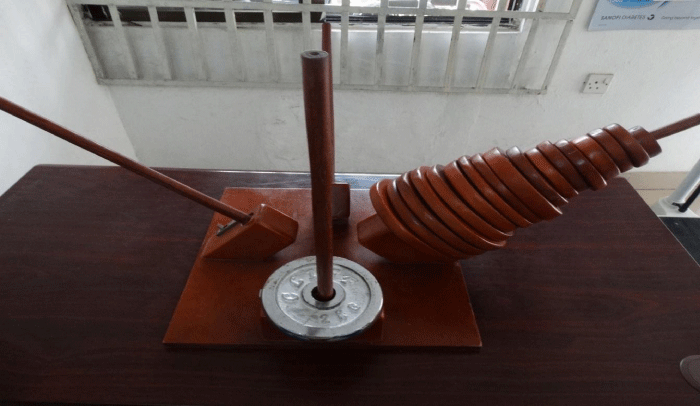
Figure 10: The inter-phalangeal joints go into extension.

Figure 11: A complete Dominic’s Physical Rehabilitation Board consisting of a wooden square board measuring 16 by 16 inches on the sides and 0.5 inch in thickness.

Figure 12: A Cerebral Palsy child in a Rehabilitation class using Dominic’s Board.
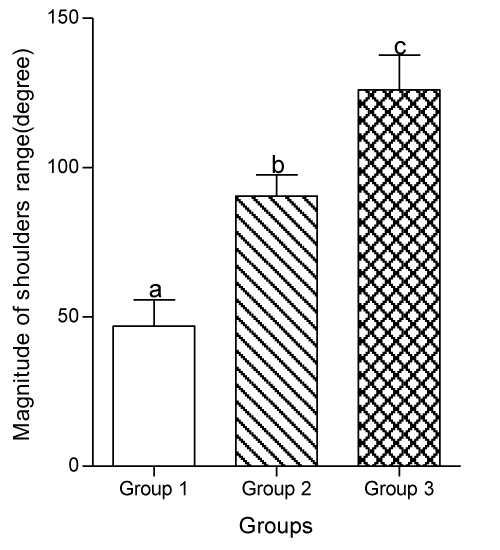
Figure 13: A Child with left Shoulder injury using Dominic’s Physical Rehabilitation Board during her rehabilitation phase.
Dominic’s physical rehabilitation board was specially designed to address some of the short falls from previous similar devices including inability to target the subject group [5], therapeutic ineffectiveness [7], high cost of home-base therapy [5]. Also, some of the previous devices selectively impact on certain joints, and has unidirectional oriented movement, whereas Dominic’s board has multiple joints involvement, and enhances movement in multiple directions.
Dominic’s board unlike others is not powered and not fixed and hence can be moved from one point to the other. It provides the patients the opportunity to engage in intense, repetitive, and coordinated movements with prompt onset, and prolonged duration. This device is simple, economical, affordable, and targets the subjects group. It can be used to provide task oriented therapy to ULMDs of different etiologies including arthritis, sport injury, post arthroscopic surgery of wrist, elbow and shoulder, carpal tunnel syndrome, cubital tunnel syndrome, radial tunnel syndrome, crush injuries, tendinitis, dupuytren’s contracture, post flexor of extensor tendon repair, fractures involving the upper limb, post peripheral neuropathies, complex regional nerve syndrome, re-plantation, tendon transfers and lateral and medial epicondylitis.
It is less expensive and can be acquired for personal use at home, and is made of material that can be obtained locally. Because it is safe and can easily be handled it doesn’t require the continuous assistance by a trained therapist, and because it can be used at home, its use has solved the problem of shorter duration of primary rehabilitation currently being experienced due to inadequate trained physiotherapist in physical rehabilitation centers [5]. It has unrestricted utilization since it doesn’t require power and special technique and no implication.
However, at variance with other similar devices Dominic’s physical rehabilitation board is passive and patients need to be active in order to initiate movement. Therefore, it is best suited for continuation of the rehabilitation, but not for initiation of movement. Also, its use is contraindicated in patients with psychiatric disorders.
CONCLUSION
Indeed, the use of Dominic’s physical Rehabilitation Board in rehabilitating patients with ULMDS is effective regardless of the etiology of the ULMDs, and especially when used in combination with conventional treatments. It is simple, portable, cost effective, uncomplicated and patient friendly.
REFERENCES
- Leah C. Exercise to reduce musculoskeletal discomfort for people doing a range of static and repetitive work. Norwich, England HSE Books, 2011.
- Filho S, Babosa S, Barreto SM. Occupational activity and prevalence of upper limb and back pain among dentists in Belo Horixonte, Minas Gerais State, Brazil: a contribution to the debate on work-related musculoskeletal disorders. Cad Saúde Pública.2001; 17: 181-193. Ref.: https://goo.gl/h8CvEc
- Lindfors P, von Thiele U, Lundberg U. Work characteristics and upper extremity disorders in female dental health workers. J Occup Health. 2006; 48: 192-197. Ref.: https://goo.gl/2z5MnP
- Turk DC, Rudy TE. Neglected factors in chronic pain treatment outcome studies-referred patterns, failure to enter treatment and attrition. Pain. 1990; 43: 7-25. Ref.: https://goo.gl/d77Oun
- Maciejasz P, Eschweiler J, Gerlach-Hahn K, Jansen-Troy A, Leonhaedt S. A survey on robotic devices for upper limb rehabilitation. J Neuroeng Rehab. 2014; 11: 3. Ref.: https://goo.gl/e55qYa
- Richards L, Hanson C, Wellborn M, Sethi A. Driving Motor recovery after stroke. Top stroke rehabiliat. 2008; 15: 397-411. Ref.: https://goo.gl/1jcBRM
- Patton J, Smal SL, Rymer WZ. Functional restoration for the stroke survivor: informing the efforts of engineers. Top Stroke Rehabil. 2008; 15: 521-541. Ref.: https://goo.gl/nRsbKh